This document discusses burn injuries including:
1) Depth and extent of burns are classified using tools like the Lund-Browder chart to determine severity. Location of burns can impact respiratory function.
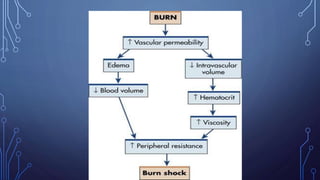
2) Emergent management focuses on airway, breathing, circulation and stopping the burning process. Fluid shifts cause hypovolemic shock in the first days.
3) Complications include cardiovascular issues like shock and respiratory issues like airway burns and inhalation injuries. Fluid replacement therapy is critical to manage fluid shifts. The Parkland formula guides initial fluid resuscitation.