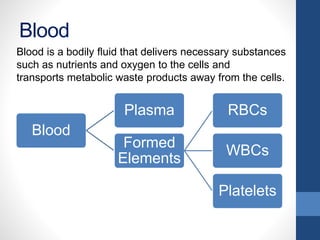
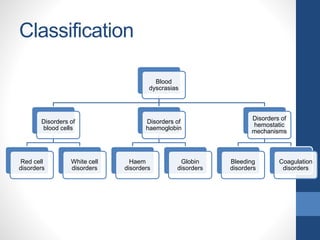
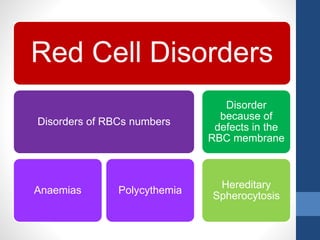
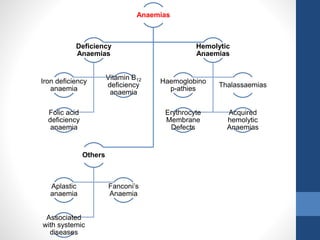
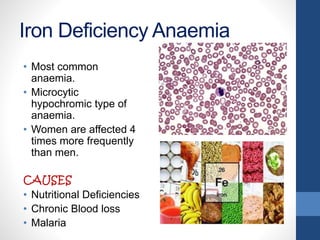
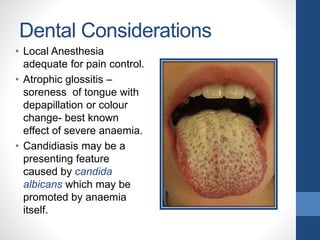
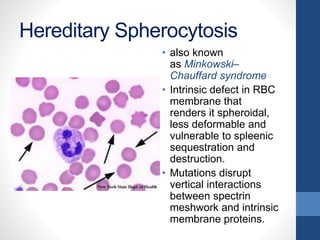
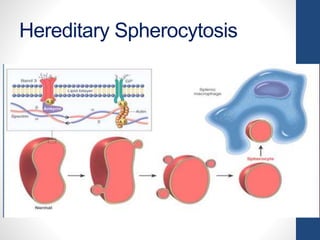
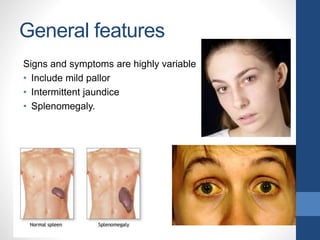
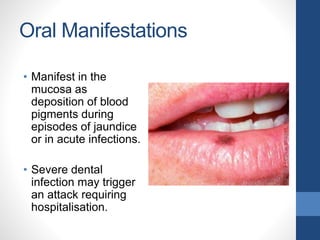
This document provides an overview of blood dyscrasias (disorders of blood cells). It begins with an introduction to dyscrasia as a concept from ancient Greek medicine meaning "bad mixture." The document then discusses the history of dyscrasias and provides classifications of blood dyscrasias including disorders of red blood cells, white blood cells, hemoglobin, hemostatic mechanisms, and more. Several specific red blood cell disorders are described in detail, including iron deficiency anemia, vitamin B12 deficiency anemia, folic acid deficiency anemia, aplastic anemia, polycythemia, and hereditary spherocytosis. Management and dental considerations are provided for many of these conditions.






























































![BLOOD DYSCRASIA [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/blooddyscrasiaautosaved-240119171311-77e8d946-thumbnail.jpg?width=640&height=640&fit=bounds)
















![BLOOD_DISORDERS-2[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/blooddisorders-21-230610142333-f4472c75-thumbnail.jpg?width=640&height=640&fit=bounds)




















