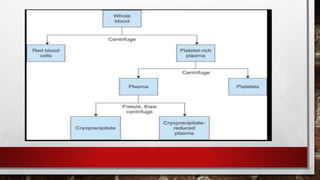
Whole blood can be separated into components which allows for optimal survival of each constituent and transfusion of only the specific component needed by the patient. This avoids unnecessary transfusion and allows blood from one donor to treat several patients. Components include red blood cell concentrate, platelet concentrate, leukocyte-reduced products, plasma components like fresh frozen plasma and derivatives, and cellular components like granulocytes.