Download as PDF, PPTX












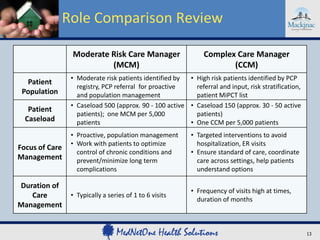




















This document discusses Michigan's Primary Care Transformation Demonstration Project. It outlines the agenda for webinar #10, including discussions on Medicaid and Medicare payments, care managers, project committees and metrics. It then provides details on performance metrics and incentives, care manager roles, clinical quality measures, and expectations for participating medical organizations. The webinar aims to update practices on the project and support development of patient-centered medical home capabilities.






























































































