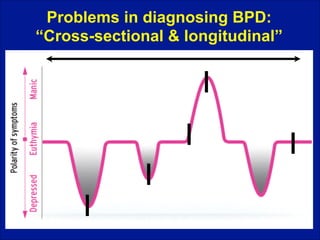
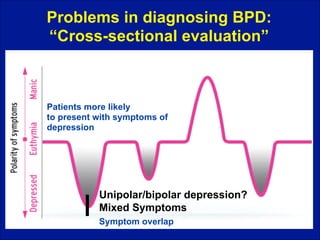
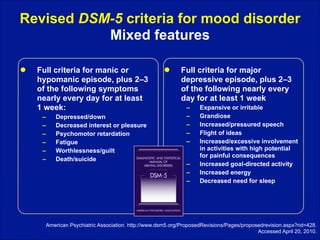
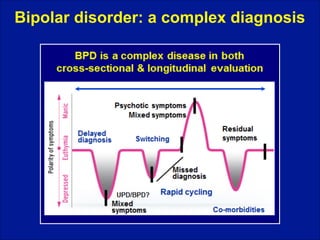
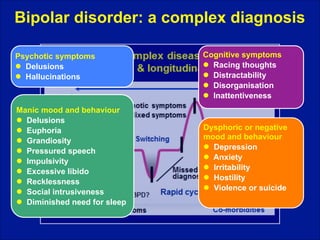
This document provides an overview of bipolar disorder and some of the challenges involved in accurately diagnosing it. It discusses how Aretaeus of Cappadocia in the 2nd century AD provided early descriptions of complex conditions including mania and melancholia. Diagnosing bipolar disorder can be difficult due to problems with cross-sectional and longitudinal evaluation of patients. Symptom overlap between unipolar depression and bipolar disorder can lead to misdiagnosis. The document examines factors that can complicate and delay an accurate diagnosis of bipolar disorder.

![Aretaeus of Cappadocia (AD 81–138)
‘‘I think that melancholia is the
beginning and a part of mania…
The development of mania is really
a worsening of the disease rather
than a change into another...
The symptoms [of melancholia] are not
unclear: [the melancholics] are
either quiet or dysphoric, sad or
apathetic. Additionally, they could
be angry without reason and
suddenly awake in panic”
Marneros & Goodwin,Cambridge University Press, 2005
ARETAEUS of Cappadocia (fl. ca A.D. 50). Libri septem - RUFUS of Ephesus (fl. 1st century A.D.) De corporis humani
partium appellationbus libri tres. in Latin by Junius Paulus Crassus (ca 1500-75). Venice: Giunta Press, 1552.](https://image.slidesharecdn.com/bipolaracomplexdisorder-140211031938-phpapp02/85/Bipolar-a-complex-disorder-4-320.jpg)