Downloaded 79 times































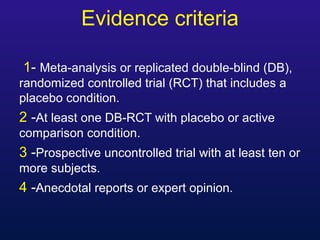







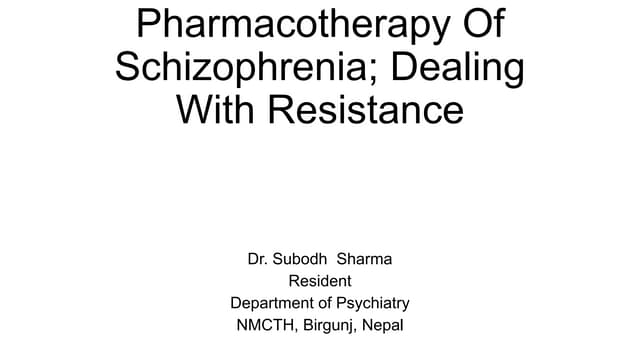
![Likely to be Beneficial [SR] Trade off
between Benefit
and Harm [SR]
Mania Monotherapy; lithium, divalproex ER,
olanzapine, risperidone, quetiapine,
quetiapine XR, aripiprazole, ziprasidone,
asenapine , paliperidone ER[A]
Combining (lithium or valproate) with
risperidone, quetiapine, olanzapine,
aripiprazole, asenapine [A]
Monotherapy:
carbamazepine,
carbamazepine ER,
Clozapine [I]
Oxcarbazepine [I] ECT,
haloperidol (A)
Combination therapy:
lithium + divalproex
Mixed
Episode
Valproate, carbamazepine,
aripiprazole, olanzapine,
risperidone, or ziprasidone [A]
Clozapine [I]
Oxcarbazepine [I]
Quetiapine [I]
Lithium [I]](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-52-320.jpg)
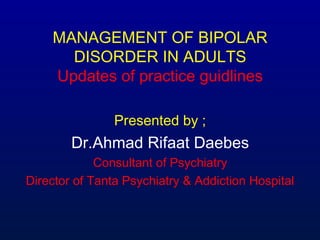
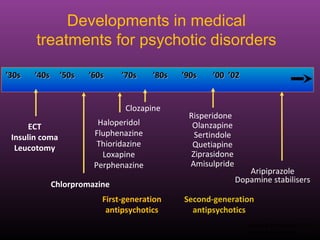
![Unlikely to be Beneficial OR May
be Harmful [SR]
Mania Monotherapy: gabapentin, topiramate, lamotrigine,
verapamil, tiagabine
Combination therapy: risperidone +
carbamazepine, olanzapine + carbamazepine
Mixed Episode Lamotrigine [D]
Topiramate [D]
Gabapentin [D]](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-53-320.jpg)



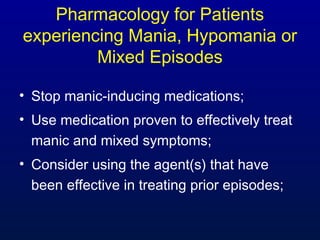

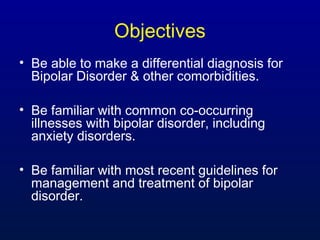
![If mania/mixed symptoms are
severe, with or without psychosis:
• Use a combination of an antipsychotic and
either Li or DVP.
• If severe mania - olanzapine, quetiapine,
aripiprazole, or risperidone [B]
• If severe mixed - aripiprazole, olanzapine,
risperidone, or haloperidol [B] and
quetiapine .](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-59-320.jpg)
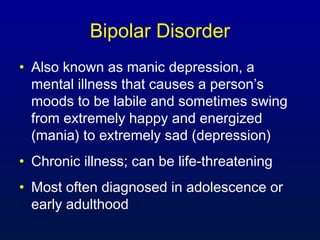
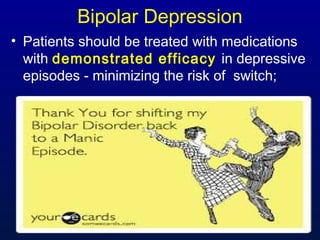
![If monotherapy is insufficient…
• ADJUST medications if there is no response
within 2 – 4 weeks on an adequate dose;
• Consider SWITCHING to another monotherapy
[I];
• Consider COMBINATION therapy (see
guidelines for choices for severe mania and/or
mixed symptoms);](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-60-320.jpg)
![Cont’d
• Consider Clozapine, particularly if it has been
successful in the past or if other antipsychotics
have failed [I];
• Electroconvulsive therapy (ECT) may be
considered [C];
• Risks and benefits of specific long-term
pharmacotherapy should be discussed prior to
starting medication and throughout all treatment
[A]](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-61-320.jpg)


![• Consider agent(s) effective in treating
prior episodes;
• Risk for mood destabilization to
mania should be monitored closely for
emergent symptoms [I];
• For patients with psychotic features, an
antipsychotic should be started [I];](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-65-320.jpg)
![cont’d
• Consider adding an evidence based
psychotherapeutic intervention to improve
adherence and patient outcome [B];
• Consider other psychiatric and medical
conditions and try to avoid exacerbating
them;
• If diabetes or obesity are present, consider
the risk and benefit of utilizing medications
that are less associated with weight gain.](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-66-320.jpg)
![Likely to be
Beneficial [SR]
Trade off between
Benefit and Harm [SR]
Acute
Depressive
Episodes
Monotherapy: lithium (B),
lamotrigine, quetiapine,
quetiapine XR (A)
Combination therapy:
Lithium with adjunctive
lamotrigine [A]
lithium or divalproex +
SSRIb,
olanzapine + SSRIb,
lithium + divalproex,
lithium or divalproex +
bupropion
Monotherapy: divalproex,
lurasidone(c)
Combination therapy:
quetiapine + SSRIb,
adjunctive modafinil, lithium or
divalproex + lamotriginec,
lithium or divalproex +
lurasidone(c )](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-67-320.jpg)
![Unknown Unlikely to be
Beneficial OR May be
Harmful [SR]
Acute
Depressive
Episode
Monotherapy:
carbamazepine,
olanzapine, ECT(D)
Combination therapy:
lithium +carbamazepine,
lithium + pramipexole,
lithium or divalproex +
venlafaxine,
lithium + MAOI,
lithium or divalproex or
AAP + TCA,
lithium or divalproex or
carbamazepine + SSRIb
+
lamotrigine, quetiapine +
Monotherapy: gabapentin,
aripiprazole, ziprasidone (c)
Combination therapy:
adjunctive ziprasidone,
adjunctive levetiracetam(c)](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-68-320.jpg)


![Recommendations for Treatment of
Depressive Episodes
• If patient is having intolerable side effects switch
to another effective treatment [I];
• Ensure that medication(s) are in therapeutic
range, and raise until improvement, side effects
or the dose manufacturer’s suggested upper
limits [I];
• If no response within 2 – 4 weeks on a good
dose then augment, switch, or consider ECT;](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-73-320.jpg)
![Cont’d
• Any discontinuation of medication should be
tapered and the patient should be monitored
for mood destabilization [I];
• If mania/hypomania/mixed symptoms occur,
go to Module A [I];
• Risks and benefits of long term
pharmacotherapy should be discussed prior
to starting medication and throughout
treatment [A].](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-74-320.jpg)
![Likely to be Beneficial [SR] Trade off between
Benefit and Harm [SR]
Monotherapy: lithium, lamotrigine (limited
efficacy in preventing mania), divalproex,
olanzapine a,
quetiapine, risperidone LAI b, aripiprazole b
Combination therapy with lithium or
divalproex: quetiapine, risperidone LAI b,
aripiprazole b, ziprasidone b
Monotherapy: carbamazepine,
palideridone ER c
Combination therapy: lithium +
divalproex, lithium +
carbamazepine, lithium or
divalproex + olanzapine,
lithium + risperidone, lithium +
lamotrigine, olanzapine +
fluoxetine
Maintenance Treatments](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-75-320.jpg)
![Maintenance Recommendations
(continued)
Maintenance benefit
unknown
Unlikely to be Beneficial
OR May be Harmful [SR]
Monotherapy: asenapine c
Combination therapy: phenytoin,
clozapine, ECT, topiramate,
omega-3-fatty acids,
oxcarbazepine,
gabapentin, asenapinec
Monotherapy: gabapentin,
topiramate, or antidepressants (d)
Combination therapy: flupenthixol](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-76-320.jpg)
![Maintenance Therapy
• A structured approach is recommended [A];
• Patients who have had an acute manic episode
should be treated for at least 6 months after the
initial episode is controlled and encouraged to
continue on life-long prophylactic treatment [A];
• Risks and benefits of long term pharmacotherapy
should be discussed prior to starting medication
and should be continued throughout treatment
[C];](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-77-320.jpg)
![Cont’d
• Patients who have had >1 manic
episode, or 1 manic and depressive
episode, or >2 depressive episodes,
should be encouraged to continue on
life-long prophylactic treatment, as the
benefits outweigh the risks [A];](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-78-320.jpg)
![• If medications are to be discontinued, they
should be slowly and GRADUALLY
TAPERED over at least a 2 to 4 week
period, unless medically contraindicated, to
prevent a “REBOUND” episode of bipolar
disorder and/or increase the risk of
suicide [B].](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-79-320.jpg)




![• Patients in remission should be seen every 1 to 3 months
with ongoing assessment of recent symptoms [I];
• All patients on medication should be monitored for potential
adverse effects [B];
• Monitor serum concentrations (as appropriate) and other
appropriate blood work every 3 to 6 months to maintain
efficacy and avoid toxicity [A/B];](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-84-320.jpg)
![• For those on APs, monitor weight, waist circumference,
blood pressure, BMI, plasma glucose and fasting lipids
[C].
• Adherence to medication therapy should be routinely
evaluated at each visit [A];
• Assess any changes in patient’s family and community
support [C].](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-85-320.jpg)
![Adjunctive Psychoeducation
• Psychoeducation should emphasize [B]:
– The importance of active involvement in
treatment
– The nature and course of their bipolar illness
– The potential benefit and adverse effects of
treatment options
– The recognition of early signs of relapse
– Behavioral interventions that can lessen the
likelihood of relapse including careful
attention to sleep regulation and avoidance of
substance misuse.](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-86-320.jpg)
![Cont’d
• With the patient’s permission, family
members or significant other should be
involved in the psychoeducation process
[C];
• A structured group format in providing
psychoeducation and care management
for patients with clinically significant mood
symptoms should be considered [A].](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-87-320.jpg)
![Adjunctive Psychotherapies
• CBT for those who have achieved remission
from an acute manic episode and who have had
<12 previous acute episodes [A];
• IPSRT for those who have achieved remission
from an acute manic episode and are
maintained on prophylactic medication [B];](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-88-320.jpg)
![Cont’d
• Structured Family therapy can be
considered for couples and families who
are coping with BD [C];
• Patients may benefit from chronic care
model-based interventions [B], especially
when more symptomatic or recently
hospitalized [A].](https://image.slidesharecdn.com/bipolarmanagement-160107171008/85/Bipolar-management-89-320.jpg)





The document provides updates on the management of bipolar disorder, highlighting the importance of accurate diagnosis, common comorbidities, and recent treatment guidelines. It emphasizes the severe health impacts and higher mortality rates faced by individuals with bipolar disorder due to inadequate treatment and recognition. Additionally, the document outlines the complex relationship between bipolar disorder and co-occurring conditions such as anxiety disorders, as well as the critical need for updated treatment strategies based on evolving clinical evidence.