The document provides an overview of bipolar disorder including:
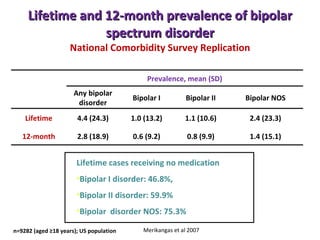
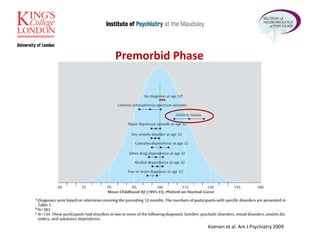
1. The lifetime and 12-month prevalence of bipolar spectrum disorders based on a large US population study.
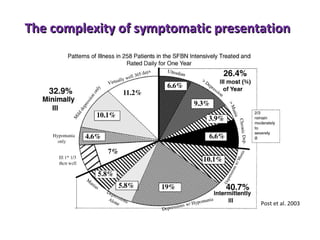
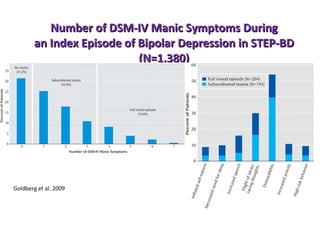
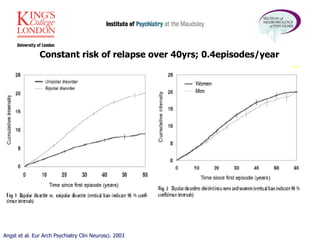
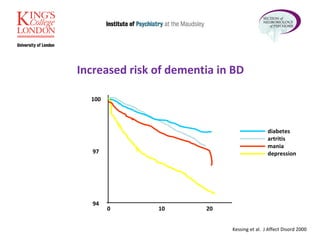
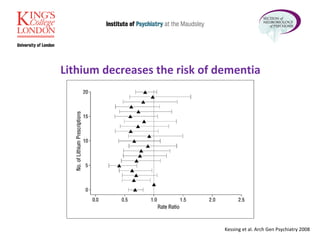
2. Bipolar disorder has a complex symptomatic presentation and patients experience a constant risk of relapse over decades.
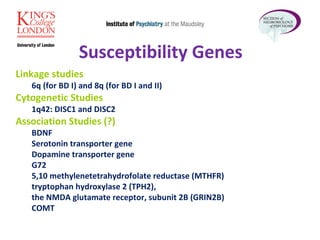
3. Genetics plays a large role in bipolar disorder liability and genome-wide association studies have identified several susceptibility genes.
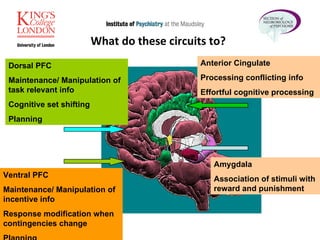
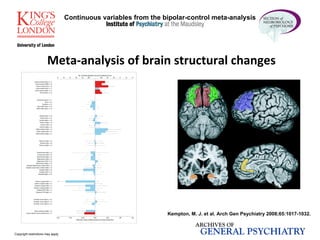
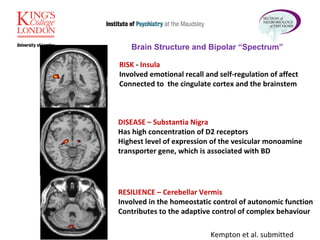
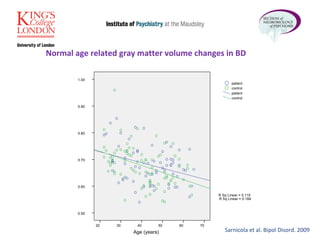
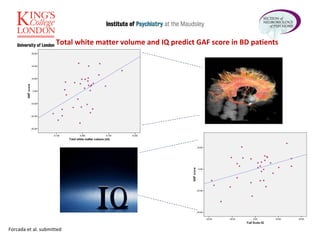
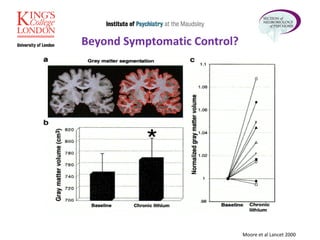
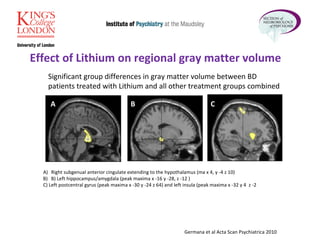
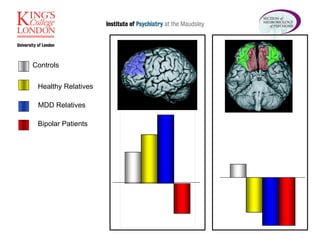
4. Structural and functional brain imaging research has found differences in bipolar patients in areas involved in emotion regulation, cognitive control, and reward processing.