The document provides an overview of biomedical waste management. It defines biomedical waste and outlines the key rules and regulations regarding its handling and disposal. The main points are:
- Biomedical waste is any waste generated during healthcare and can be hazardous to health and the environment if not properly managed.
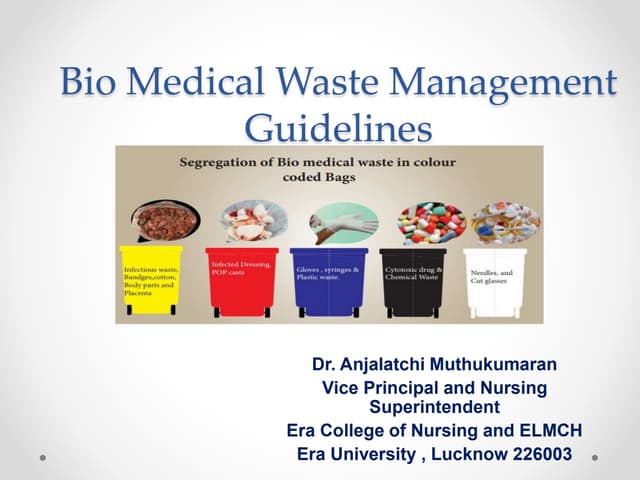
- The Bio Medical Waste (Management and Handling) Rules classify waste into 10 categories and specify treatment and disposal methods for each.
- Key responsibilities include appropriate segregation, storage, transportation, and treatment of waste according to the rules before final disposal.
- Common treatment methods include incineration, autoclaving, chemical disinfection, and secured landfilling. Proper training and safety measures for