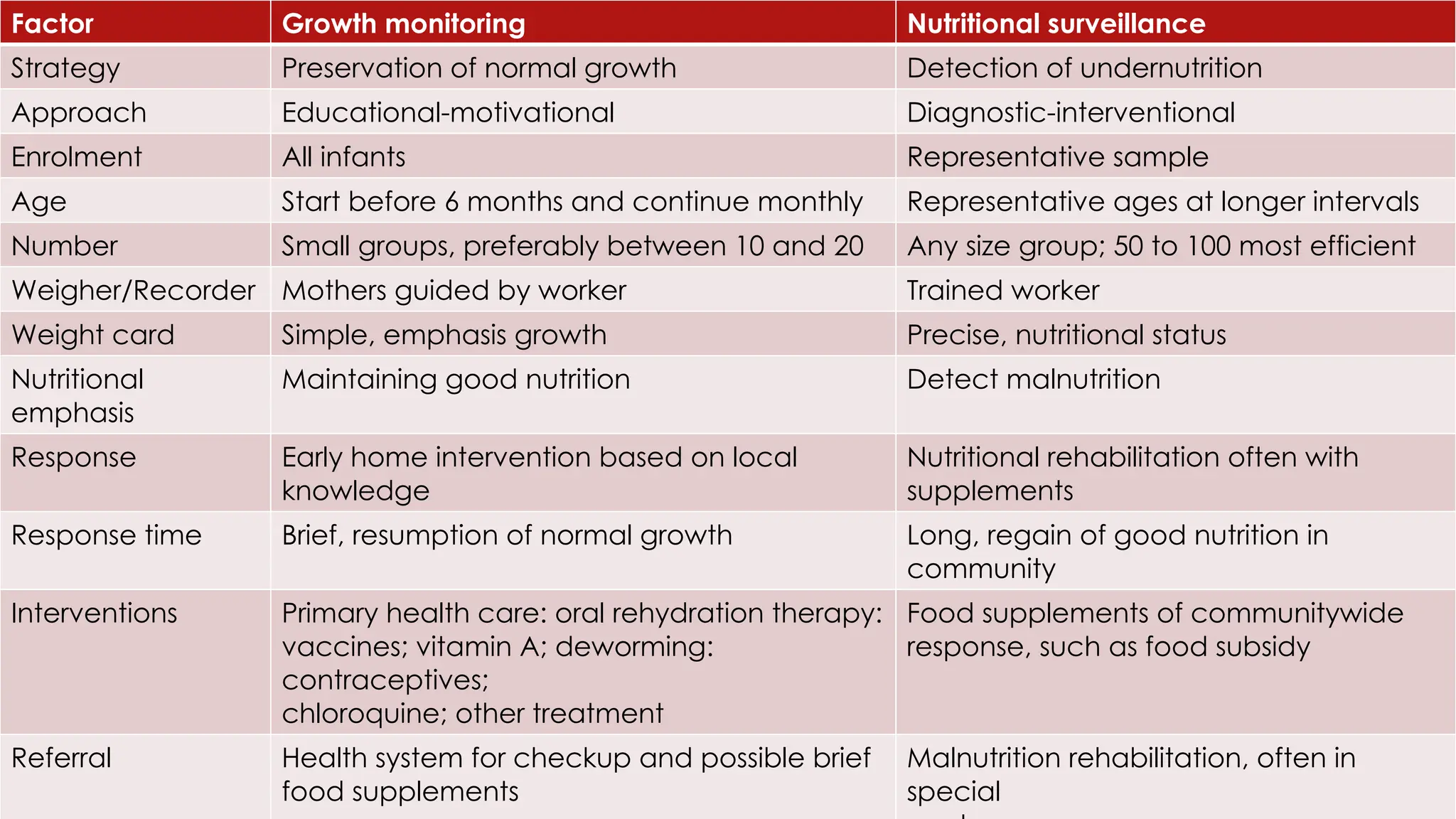
The document outlines nutritional surveillance methods, emphasizing the collection and analysis of data on population nutrition and malnutrition risk factors. It distinguishes between nutritional surveillance and growth monitoring, detailing various data collection approaches and the importance of indicators for assessing nutritional status. Additionally, the text discusses the multifaceted nature of malnutrition, including its direct and indirect effects, and highlights the socio-cultural and ecological aspects influencing nutritional health.