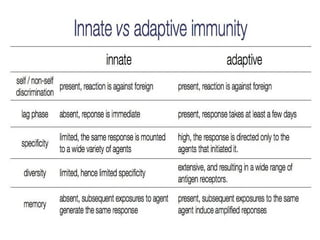
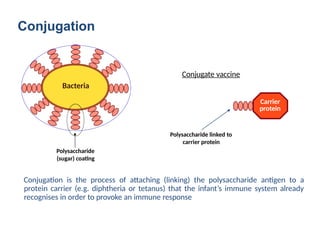
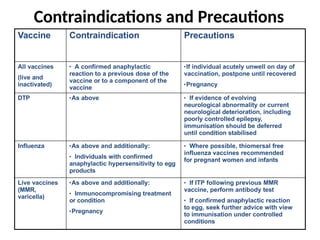
The document covers adult immunization, detailing the immune system's role in infection defense and the two types of immunity: innate and adaptive. It outlines immunization methods, including vaccines and their administration routes, types of vaccines (live, inactivated, conjugate), and recommendations for various diseases prevalent in India. Additionally, it discusses challenges facing adult immunization, such as funding, knowledge gaps, and public health infrastructure issues.