Bioequivalence Study.pptxDiscusses bioequivalence study its applications & study designs
1.
Bioequivalence Study
Presenter: Dr.Pragya Pandey (JR-2)
Department of Pharmacology & Therapeutics
King George’s Medical University
Lucknow, Uttar Pradesh, India.
Email – drpragyakgmu@gmail.com
2.
Contents
• WHO definitionof bioequivalence
• Need for bioequivalence study
• Biowaiver
• Methods
• Prerequisites
• Study designs
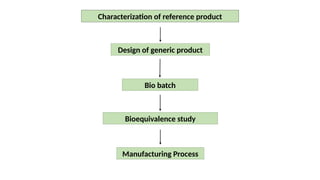
• Flowchart
• Summary
3.
Specific learning objective
Afterthe teaching learning session, audience shall be able to
• Define bioequivalence study
• Differentiate between biosimilars and bioequivalents
• Enumerate applications of bioequivalence study
• Understand study design for bioequivalence study
4.
Abbreviations
• CDSCO: CentralDrugs Standard Control Organisation
• BCS: Biopharmaceutics Classification System
• DCGI: Drug Controller General of India
• FDA: Food and Drug Administration
• API: Active Pharmaceutical Ingredient
5.
Definition
“Two pharmaceutical productsare bioequivalent, if they are
pharmaceutically equivalent or pharmaceutical alternatives, and their
bioavailabilities, in terms of rate and extent of absorption, after
administration of the same molar dose under the same conditions, are
similar to such a degree that their effects can be expected to be
essentially the same”.
Ref: World Health Organization
6.
Biosimilars
• Biologics arelarge complex molecules made from living organisms
• Biosimilars are made taking biologics as their reference product
• Biosimilars are more complex and larger molecules compared to
bioequivalents
• Examples of biosimilars are monoclonal antibodies, insulin analogues
8.
Need for bioequivalencestudy
• Development of generic drugs
• Development of different dosage form of a drug
• For change in more appropriate marketed formulation of a drug
• To monitor manufacturing processes of drug
9.
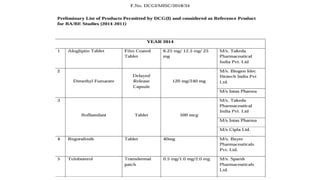
Reference product
• Referenceproduct should be the innovators product for which generic
product is made
• In absence of innovators product, Indian product approved by CDSCO
can be taken as reference product
• CDSCO releases list of approved reference product list
11.
Test Product
• Itis the representative of the product to be marketed
• It originates from a batch of 1/10 of production scale or 100,000 units
whichever is greater
• If there are multiple strengths, bioequivalence of highest strength is
established
12.
Biowaiver
• It meansin vivo bioavailability/bioequivalence studies can be waived
• It is applicable when test drug & reference product are identical and
belong to the class I & III of BCS
• BCS provides surrogate evidence for in vivo bioequivalence study
13.
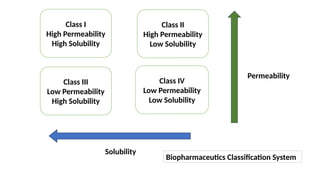
Class I
High Permeability
HighSolubility
Class II
High Permeability
Low Solubility
Class III
Low Permeability
High Solubility
Class IV
Low Permeability
Low Solubility
Permeability
Solubility
Biopharmaceutics Classification System
14.
Examples for biowaiver
•BCS class I & III drugs
• Prodrug is converted to active metabolite & the metabolite is of BCS class I &
III
• Minor changes to additives (colorant, flavoring)
• Scale up changes
15.
Advantages of Biowaiver
•Reduces time of study
• Simplifies protocol approval
• Reduces human testing
• Cost effective
Pre-requisites
• Form 44– the application for the study
• Form 12 – application for import of drug substances
• Challan receipt as required
• Details of the test drug and reference product
• Details of manufacturer of reference product
19.
Pre-requisites (cont.)
• Documents:Study protocol, Informed consent form, Undertaking by
investigator
• Ethics committee approval
• The study center should be registered under central licensing
authority
• Grant of permission from DCGI
22.
Study designs
Following typesof study designs are commonly used
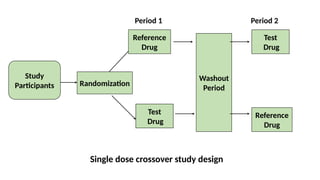
1. Single dose 2 period/2 treatment cross-over design
2. Parallel study design
3. Replicate design
23.
Cross over studydesign
• Participants are treated with both reference & test drug
• Washout period is provided in between the treatments
• Useful in study of drugs used for chronic diseases
• Used for drugs with shorter half life
24.
Cross over studydesign (cont.)
• Advantages include lesser chances of variations as participants serve
as their own control & lesser no of participants needed
• Disadvantages include longer study duration , more drop outs and
difficult to follow up and complex study
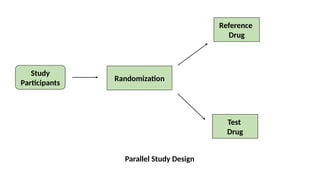
Parallel study design
•It is the traditional & commonest study design
• Participants are treated with either reference drug or test drug
• Washout period is not needed in the study
• Used for drugs with longer half life
27.
Parallel study design(cont.)
• Advantages include easy to implement study design and less chances
of drop outs
• Disadvantage is can cause inter individual variations
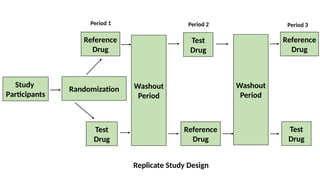
Replicate study design
•Participants are given both reference and test drug multiple times
• There is a washout period in between the treatment periods
• It can be partial or fully replicate study
• It is done for drugs with high pharmacokinetic variability
30.
Replicate study design(cont.)
• Disadvantages include longer study duration, complex study and
chances of more drop outs
• Advantages include fewer participants needed and less chances of
variations
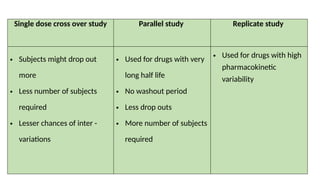
Single dose crossover study Parallel study Replicate study
• Subjects might drop out
more
• Less number of subjects
required
• Lesser chances of inter -
variations
• Used for drugs with very
long half life
• No washout period
• Less drop outs
• More number of subjects
required
• Used for drugs with high
pharmacokinetic
variability
33.
Study Conditions
• Tominimize confounding factors standardization of study
environment is ensured
• Fasting condition: overnight pre dose fasting & 4 hours post dose
for single dose study
2 hours predose & post dose for multiple dose study
• Fed condition: high fat breakfast (50% of total caloric content) 15 min
pre dose
34.
Selection of participants
•Healthy volunteers are commonly enrolled as participants
• In case of drugs with high risk of side effects, patients can be included
• Participants usually are of age 18-55 years
• Either gender can participate based on study criteria
• Women on oral contraceptives not included in study
• Teratogenic drug study should not be done on females
35.
Tests for bioequivalence
•Plasma level study
• Urinary excretion study
• Pharmacological end-point study
• Clinical end-point study
• In vitro tests for solubility & permeability
36.
Criteria for bioequivalence
•The average bioavailability of test formulation should fall between 80-
125% range of the reference (80/125 rule)
• The average bioavailability of test formulation should fall within ± 20%
of the reference (± 20 rule)
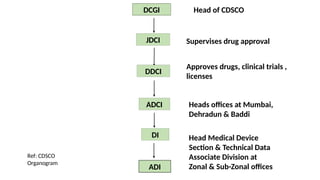
DCGI
JDCI
DDCI
ADCI
DI
ADI
Head of CDSCO
Supervisesdrug approval
Approves drugs, clinical trials ,
licenses
Heads offices at Mumbai,
Dehradun & Baddi
Head Medical Device
Section & Technical Data
Associate Division at
Zonal & Sub-Zonal offices
Ref: CDSCO
Organogram
41.
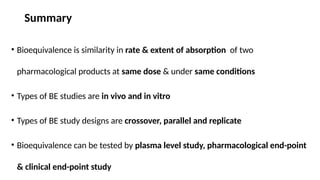
Summary
• Bioequivalence issimilarity in rate & extent of absorption of two
pharmacological products at same dose & under same conditions
• Types of BE studies are in vivo and in vitro
• Types of BE study designs are crossover, parallel and replicate
• Bioequivalence can be tested by plasma level study, pharmacological end-point
& clinical end-point study
42.
References
• Maiti R,Postgraduate topics in pharmacology.3rd
ed. Paras Medical
Publisher;2023.
• Niazi S, Handbook of bioequivalence testing. Informa healthcare;2007.
• Sarkar S, Srivastava V, Mohanty Postgraduate pharmacology.2nd
ed. Paras
Medical Publisher;2024.p.341-345
43.
Questions
• What isbioequivalence?
• What is the need of bioequivalence study?
• What is biowaiver?
• What are the types of study designs for bioequivalence studies?



































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)

















