Download to read offline







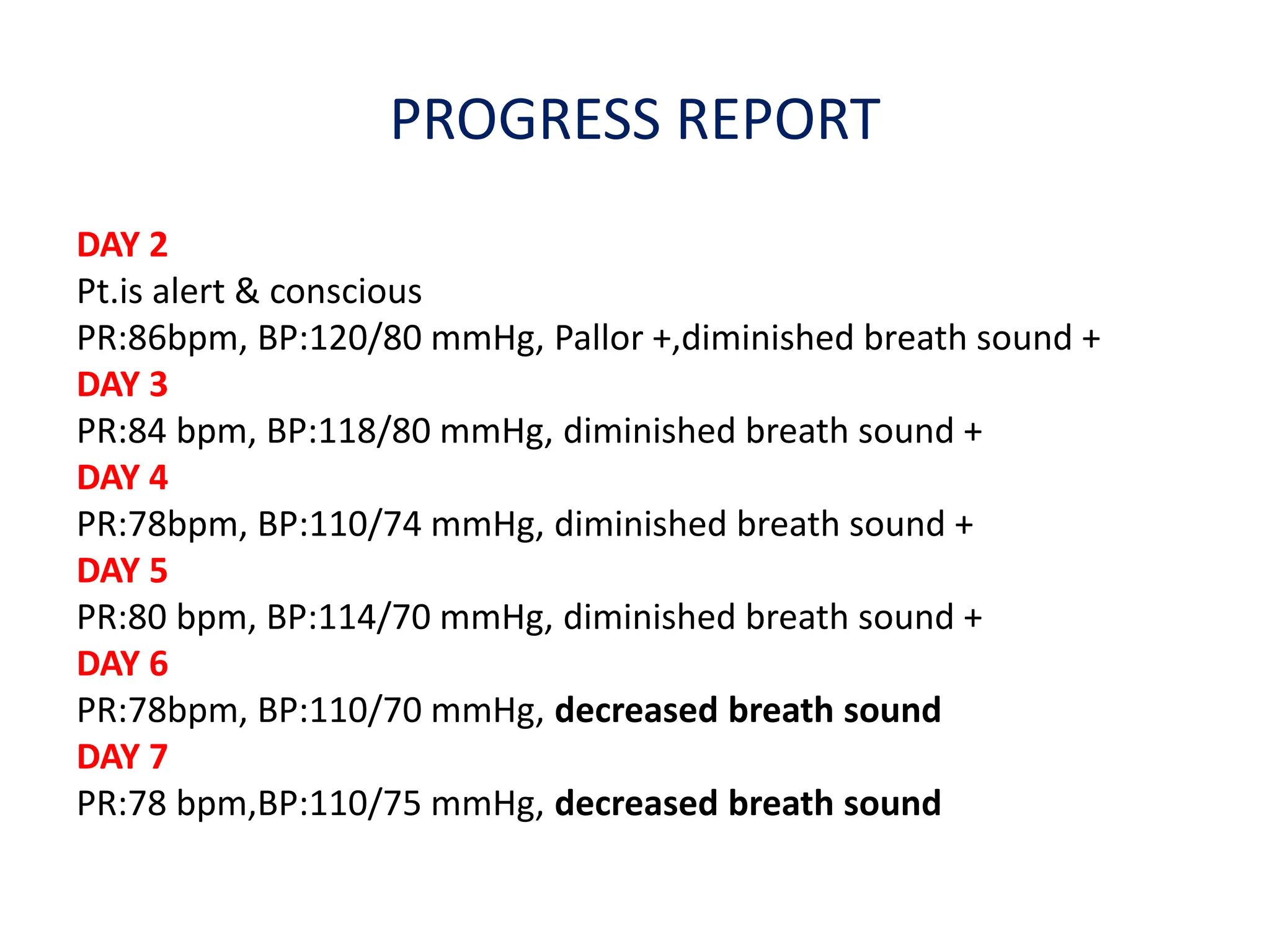
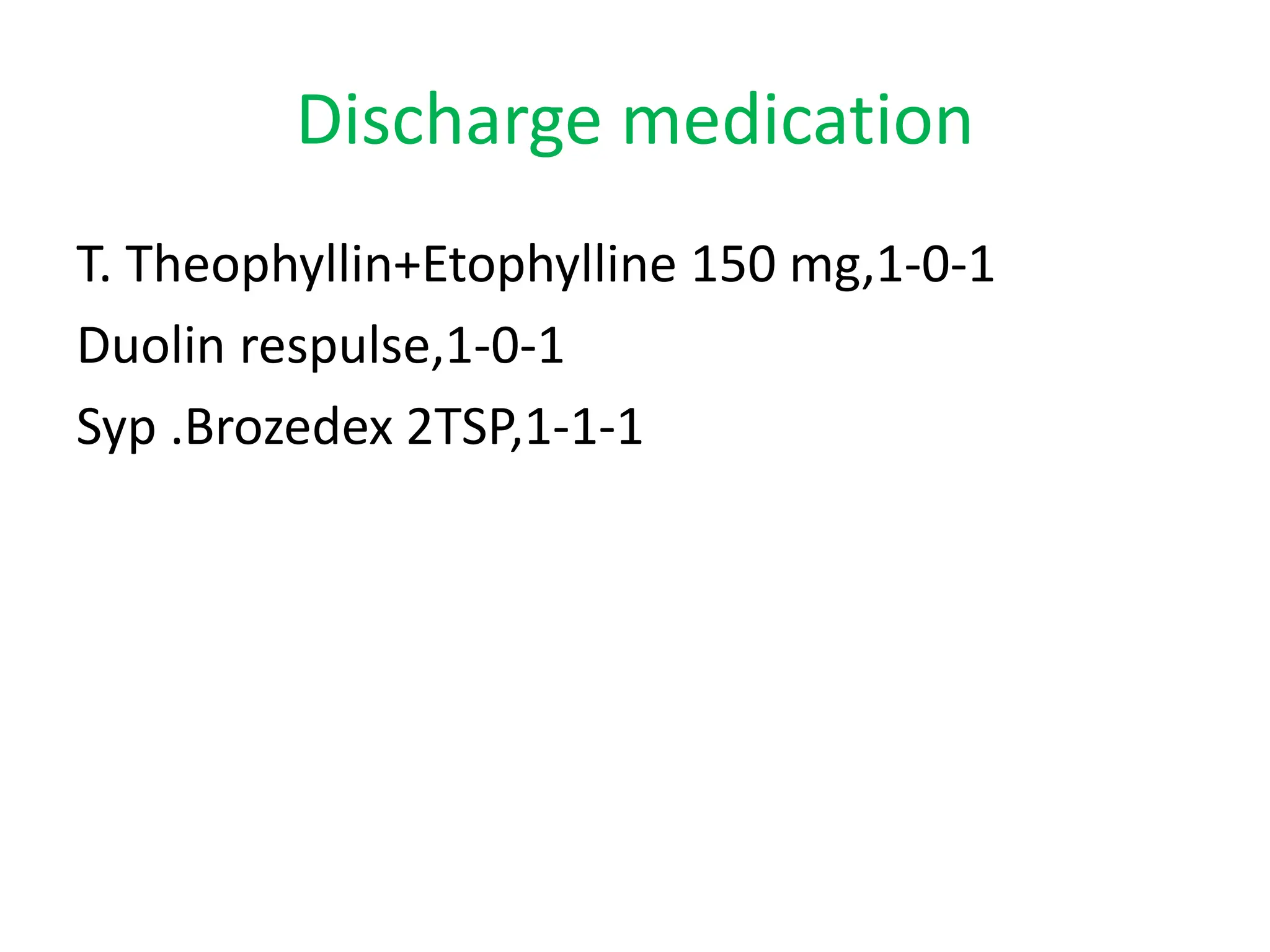





This case presentation describes a 51-year-old male patient admitted to the hospital with a diagnosis of chronic obstructive pulmonary disease (COPD). The patient presented with a 2-3 year history of cough with whitish, mucoid sputum that is occasionally blood-tinged, as well as right-sided chest pain. Physical examination revealed diminished breath sounds and mild pallor. The patient was started on medications including bronchodilators, corticosteroids, antibiotics, and theophylline. Over the course of his hospital stay, his vital signs and breath sounds improved. Upon discharge, he was prescribed continuing medications and counseling on smoking cessation, breathing exercises, and medication adherence for his long-term COPD























































































