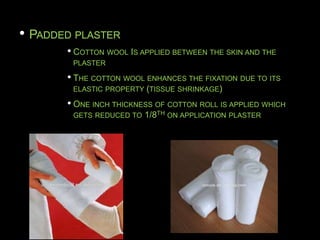
The document provides information on basic trauma management and casting in emergency settings. It discusses principles of casting including immobilization and maintaining function. It describes the two types of fracture healing and the three R's of casting - reduction, retention, and rehabilitation. Details are given on the history and uses of plaster of Paris as well as the chemical process that occurs when it is mixed with water. Guidelines are provided on the application of plaster casts and synthetic casts, potential complications, and instructions to give patients.