WOUND HEALING
By: Dr.Lucy Shitahun
‘Healing…is not a science but the intuitive art of wooing nature’
W.H. Auden, “The art of healing”
2.
Wound Healing 2
Wound
•A wound is any violation of live tissue integrity
• It can be open or closed
• Acute or chronic
• Clean, contaminated, clean-contaminated or dirty
3.
Wound Healing 3
WoundHealing
• Is the repair or reconstitution of a defect in an organ or tissue, commonly
the skin
• Represents the response of an organism to a physical disruption of a
tissue/organ, to re-establish homeostasis of that tissue/organ and stabilize
the entire organism's physiology
4.
Wound Healing 4
•Two processes by which re-establishment of homeostasis occurs
1. The process of scar formation
- Substitution of a different cellular matrix
2. The process of regeneration
- Recapitulation of the developmental processes that initially created the
injured organ
- The architecture of the original organ is re-created
5.
Wound Healing 5
Woundcan heal with…
1. Healing by primary intention
2. Healing by secondary intention
3. Healing by tertiary intension
Wound Healing 7
HEMOSTASIS
•Blood loss is prevented by vasoconstriction and formation of hemostatic
blood clot
• Vasoconstriction occurs to limit blood loss under the effects of vasoactive
mediators
• Exposed subendothelium, including collagen and tissue factor, activates
platelet aggregation and leads to clot formation (primary plug)
Wound Healing 9
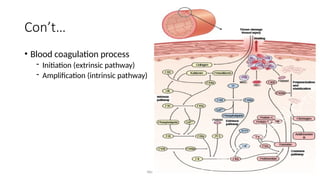
Con’t..
•Thrombin
- Fibrinogen to fibrin
- Promote platelet aggregation
- Activates other components of coagulation cascade (Factor V & VIII)
- Function as interface between hemostasis and inflammatory phase
• Proinflammatory effects of thrombin
- Stimulation of vasodilation
- Induces release of proinflammatory cytokines by endothelial cells and monocytes
10.
Wound Healing 10
Bloodclot
• A dynamic structural matrix containing functionally active proteins
and cells
• Its formation is initiated by cleavage of fibrinogen into fibrin
• Fibrin entraps platelets which adheres to the sub-endothelium by
integrins (adhesion molecules)
• Function
- Physically helps plug the wound, minimizing blood loss
- First aid against microbial invasion
- Provisional matrix for homing of blood born cells
11.
Wound Healing 11
INFLAMMATORYPHASE
• Begins immediately following tissue injury
• Meant to prepare the wound site for wound closure
• Gives rise to
- Rubor (Redness)
- Tumor (Swelling)
- Calor (Heat)
- Dolor (Pain)
Wound Healing 13
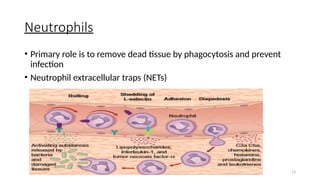
Neutrophils
•Primary role is to remove dead tissue by phagocytosis and prevent
infection
• Neutrophil extracellular traps (NETs)
14.
Wound Healing 14
Con’t…
•They also release a variety of proteases to degrade remaining ECM to
prepare the wound for healing
• Their absence does not appear to prevent the overall progress of
wound healing
• Their prolonged persistence in the wound has been proposed to be a
primary factor in the conversion of acute wounds into non-healing
chronic wounds
• Dying neutrophils are recognized by macrophages and phagocytosed
15.
Wound Healing 15
Monocyte/Macrophages
•Appear 48 to 72 hours post-injury
• Regulate both early and later stages of wound repair
• By 3 days they are the predominant cell type in the healing wound
• Phagocytose debris and bacteria
• Deliver growth factors
• Unlike the neutrophil, the absence of monocyte/macrophages has severe
consequences for healing wounds
Wound Healing 17
MastCells
• Recognize pathogens and regulate immune response
• Their number increases after 48hrs
• Trigger and modulate inflammatory stage proliferation of connective
cellular elements
• Remodeling of connective tissue matrix
• Deficit results in impaired wound healing
18.
Wound Healing 18
Lymphocyte
•Is the last cell to enter the wound
• Enters between days 5 and 7 post-wounding
• Its role in wound healing is not well defined
• Stimulatory CD4 and inhibitory CD8 cells may activate subsequent
proliferative phase
19.
Wound Healing 19
Resolutionof Inflammation
• For inflammation to stop
- Further leukocyte recruitment must be halted
- Removal of leukocyte from inflammation site
• There are lipid mediators that counter regulate excessive acute
inflammation
• Sustained inflammatory response could be induced by microbial
biofilms
20.
Wound Healing 20
PROLIFERATIVEPHASE
• Starts around 2 days and lasts 3 weeks
• Overlaps with inflammatory phase
• Supports
- Re-epithelialization
- Formation of new blood vessels
- Influx of fibroblasts and lying down of ECM
21.
Wound Healing 21
Granulationtissue
• Is a perfused, fibrous connective tissue that grows from the base of
the wound
• Replaces fibrin clot
• Able to fill wound of any size
• Light red or dark pink in color
• Serves as a bed for tissue repair
22.
Wound Healing 22
Con’t…
•Granulation tissue is composed of three cell types: fibroblasts,
macrophages, and endothelial cells
• These cells form ECM and new blood vessels
• Keratinocytes adjacent to the wound alter their phenotype and
migrate laterally
• Keratinocytes restore epithelial continuity
23.
Wound Healing 23
Con’t…
•Fibroblasts produce the ECM
• ECM will be the most visible component of cutaneous scars
• In proliferative phase, the provisional matrix of fibrin is replaced with
thinner type III collagen, which will in turn be replaced by thicker type I
collagen during the remodeling phase
24.
Wound Healing 24
Vascularization
•Via angiogenesis or vasculogenesis
• Regulated by all phases of wound healing
• Proangiogenic factors that are released by macrophages include VEGF,
fibroblast growth factor 2, angiopoietin 1, and thrombospondin
Once collagen matrix has filled in the wound cavity, fibroblasts
rapidly disappear and newly formed blood vessels regress, resulting in
a relatively acellular scar
25.
Wound Healing 25
REMODELINGPHASE
• last from 21 days up to 1 year
• Begins with the programmed regression of blood vessels and
granulation tissue
• characterized by the processes of wound contraction and collagen
remodeling
• Wound contraction is produced by wound myofibroblasts,
26.
Wound Healing 26
Con’t…
•Replacement of type III collagen by type I
• Mediated by a class of enzymes known as matrix metalloproteinases
• MMPs are secreted by macrophages, fibroblasts, and endothelial cells
• Wounds will ultimately only possess 70% to 80% of the breaking
strength of unwounded skin at 1 year
27.
Wound Healing 27
Factorsthat affect wound healing
Local
• Necrotic tissue
• High bacteria burden
• High level of MMPs
• Growth factor trapping/deficiency
• Tissue hypoxia
• Repeated trauma
• Hx of irradiation
Systemic
• DM
• Anemia
• Malnutrition
• Medications
• Age
• Obesity
• Smoking
28.
Wound Healing 28
ABNORMALWOUND HEALING
• Inadequate Regeneration
- Classic example of this is found in central nervous system injuries
- Absence of neural regeneration is compensated by replacement with scar tissue
• Inadequate Scar Formation
- Examples include diabetic foot ulcers, sacral decubiti, and venous stasis ulcers
- Defects can be in the inflammatory, proliferate, or remodeling phases of wound
healing
29.
Wound Healing 29
Con’t…
•Excessive Regeneration
- They often occur in peripheral nerve-like tissue, such as peripheral nerve
regeneration leading to neuroma
- Other examples include hyperkeratosis that occurs in cutaneous psoriasis or
granuloma formation in healing wounds
- Therapeutic measures are targeted toward decreasing cellular proliferation
30.
Wound Healing 30
ExcessiveScar Formation
• Classified as either hypertrophic scarring or keloid formation
• pathophysiology remain unknown
• Decreasing the process of scar formation is the prime goal of therapy
for both disease states
• Modalities employed include steroid injections, pressure therapy with
silicone sheeting, and external beam irradiation
• Recurrence rate = 75%
31.
Wound Healing 31
•Keloids
- Are less common; <6%
- Have a genetic component
- Overgrowth of dense fibrous tissue beyond the borders of the original wound
• Hypertrophic scars
- Dense collagen fibers that do not extend beyond the original wound margins
- Are more prone to forming disabling contractures
- Are a near-universal outcome following extensive deep burn injury
Wound Healing 33
MUSCLEHEALING
• Phases of muscle healing
1. Destructive phase
• days 0 to 7 following injury
• Analogous to inflammatory phase of skin healing
• Inflammatory response with cytokine release
34.
Wound Healing 34
Con’t…
2.Repair phase
• starting at day 3
• Regeneration of disrupted myofibers
• Production of connective tissue scar
3. Remodeling phase
• Vascular ingrowth
• Regeneration of intramuscular nerves
• Adhesion of myofibers to ECM
35.
Wound Healing 35
BONEHEALING
1. Primary (direct) bone healing by surgical fixation
• Minimal callus formation
• Lamellar bone formation parallel to the long axis of the bone
2. Secondary (indirect) bone healing by external splint/cast fixation
• Typical callus formation
• Immobilization is important to allow for healing
36.
Wound Healing 36
Phasesof bone healing
1. Inflammatory phase
• from time of fracture
• Initial platelet degranulation and contained hematoma aids in healing
• osteoclasts break down necrotic bone edges, releasing osteogenic cytokines
37.
Wound Healing 37
Con’t…
2.Reparative phase
• Inflammatory debris is cleared by macrophages
• Vascular ingrowth from periosteum and endosteum
• Formation of newly woven bone at the edges
• At 3 weeks callus fills in between the edges
38.
Wound Healing 38
Con’t…
3.Remodeling phase
• Woven bone is slowly replaced by the lamellar bone
• “Clinical healing” occurs in most bones by 4 to 6 weeks
• Radiographic healing -- 6 months.
39.
Wound Healing 39
TENDONHEALING
• Two mechanisms of tendon healing categories
1. Intrinsic healing
• Tendon’s intrinsic capacity to heal
• Mediated by tenocyte/fibroblast population that arises from the tendon and
epitenon
• Relies on synovial diffusion for nutrition
• Enhanced by mobilization
40.
Wound Healing 40
Con’t…
2.Extrinsic healing
• Surrounding soft tissue’s tendency to repair damaged tendon
• Ingrowth of inflammatory cells and fibroblasts overlying the sheath
• Immobilization*
41.
Wound Healing 41
Phasesof healing
1. Inflammatory phase
• Tendon defect fills with hematoma, tissue debris, and fluid
• Both intrinsic cells and cells that have migrated from the periphery bridge the
defect
• Increased phagocytic activity clears necrotic debris
42.
Wound Healing 42
Con’t…
2.Proliferative phase
• Fibroblasts are the predominant cell type
• Strength of repair begins and increases at ~2 to 3 weeks
• Synovial sheath is reconstituted at 3 weeks
• Vascular ingrowth occurs
43.
Wound Healing 43
con’t…
3.Remodeling phase
• Collagen fibers continue to realign to the long axis of the tendon
• Fibers realigned by 8 weeks
#1 Wound healing is a natural restorative response to tissue injury
Healing is a interaction of a complex cascade of cellular events that generates resurfacing, reconstitution and restoration of the tensile strength of injured skin
#2 It is believed that healthy skin can regenerate and repair itself under most common conditions
Open: lacerations, puncture, abrasion, avulsion, amputation
Closed: contusions due to blunt trauma
An acute wound is a wound for which the injury has occurred within the past 3 to 4 weeks
If the wound persists beyond 4 to 6 weeks, it is considered a chronic wound
a chronic wound also represents wounds that have been present for months or years. "Non-healing, recalcitrant," and "delayed healing" are terms used interchangeably to describe chronic wounds
#4 Scar formation refers to the patching of a defect with a different or modified tissue (i.e. scar)
Tissue regeneration refers to the complete re-creation of the original tissue architecture
A balance between scarring and tissue regeneration is unique to different tissues and organs For example, neural injury is characterized by little regeneration and much scarring, whereas hepatic and bone injury usually heals primarily through regeneration. It is important to note, however, that the liver can respond to injury with scarring as it does in response to repetitive insults during the progression of alcoholic cirrhosis
#5 There are 3 general techniques of wound treatment
Healing by primary intention - incisional wounds that are re-approximated by sutures in the absence of complications
Healing by secondary intention
Wounds that are left open (for any reason)
Defect is filled in with granulation tissue and then re-epithelialized
Have a higher likelihood of progressing to a chronic wound
Tertiary intension – wound left open for a no. of days and closed when it is clean
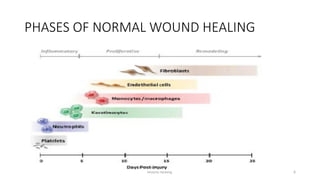
#6 Healing is a systemic process traditionally explained in terms of 4 overlapping classic phases: hemostasis, inflammation, proliferation (granulation) and maturation (remodeling)
#7 For bleeding wounds the highest priority is to stop bleeding and this is achieved by hemostasis
It is a protective physiological response to vascular injury and Starts within the first moments of the injury
Vasoactive mediators (epinephrine, norepinephrine, PG and TX) causing temporarily blanching of the wound
#8 Extrinsic pathway – tissue factor , factor 7
Intrinsic pathway – plasma factor 8,9 & 11
TF is expressed by adventitial cells surrounding blood vessels and it initiates clotting, and it is expressed within platelets
When there is an injury to blood vessels F7 comes in contact with TF (expressed in TF bearing cells Eg: WBC),
the TF-F7 complex will activate F9&10, activated F10 with its cofactor 5 forms prothrombinase complex which changes prothrombin to thrombin
#9 -Thrombin changes the soluble fibrinogen into insoluble fibrin
-Continues with the intrinsic pathway, the intrinsic pathway begins with formation of primary complex on collagen
-vasodilation results in plasma extravasation, edema, inc of endothelial cell adhesion molecules
-endothelial cells (IL 6,8 & CCL2), monocytes (IL6,1B, TNF)
#10 Primarily made up of fibrin, cells (erythrocytes & platelets), ECM protein (fibronectin, vitronectin & thrombospondin)
Once platelets are trapped in fibrin they release granules which fun as a reservoir for biologically active proteins (RATES, thrombin, TGF-ß, PDGF, VEGF)
Fibrin binds to FGF-2 & VEGF for wound angiogenesis and binds to ILGF and promote stromal cell proliferation
Blood born cells – inflammatory cells, stem cells, progenitor cells
Provisional matrix is enriched in cytokines and growth factors that regulate function of homing cells
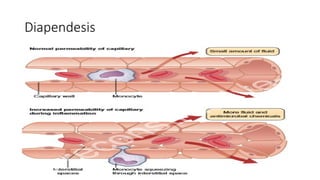
#12 The proinflm. Cytokines that are released by platelets will activate the local blood vessels leading to vasodilation and inc. permeability
In this process of diapendesis there will be extravasation of inflammatory cells like neutrophils and monocytes
There will also be extravasation of fluid causing edema
In infected wound bacterial products enhance neutrophil recruitment to the wound site
#13 -For the first 2 days following wounding, there is an impressive infiltration of neutrophils
-Phagocytosis occurs with NETs, complement/abs coated microorganisms bind to receptors on the surface of phagocytes – invagination of cell membrane – inc O2 consumption which is converted to high reactive O2 species (Respiratory burst), cytokine granules discharge their contents in to the phagosome theat results in death of the ingested microorganism
#14 Antimicrobials are also delivered by neutrophils to the wound
Balance b/n neutrophil released protease level and intrinsic inhibitors in the wound is important for wound healing progression
Chronic wounds have elevated levels of neutrophil derived proteases, specially MMPs, which is inhibited by TIMPs in normal wounds (low level in chronic wound resulting in persistent neutrophil release)
In a healing wound neutrophil infiltration ceases after few days of injury, expended neutrophils are programmed to die,
#15 They are recruited to healing wounds primarily by expression of monocyte chemoattractant protein 1
Monocytes extravasate through the blood vessel through the ECM in to the wound and differentiate to macrophages
Macrophages fun as antigen presenting cells and phagocytes (dead cells and debris), also deliver a wide range of growth factors (TGF, VEGF, PDGF) which are used for cell proliferation, synthesis of ECM and induction of angiogenesis resulting in wound healing
#16 M2 – role is to resolve inflammation
Diabetic wound – have impaired ability to phagocytose apoptotic cells which prevents switch from M1 to M2 phenotype , macrophages have persistent inflammatory state
#17 Are well known for their control role in mediating allergic response. Beyond that fun it is also known that mast cells are physiologically significant in recognizing pathogens and in regulating immune response.
In response to injury mast cells at the wound site degranulate within hrs and become histologically silent but after 48 hrs they are seen again and thir no. inc as healing progresses
#19 The inflammatory response is only helpful to the healing process if they are timely and transient. If its disregulated it prevent progression of wound healing cascade beyond inflammatory phase
Bacterial biofilms promote pro-inflammatory response
#20 By this time degradation of fibrin clot by macrophages has began and endothelial cells and fibroblasts fill the space
This fibroblasts produce cytokines that induce keratinocytes to migrate and proliferate inducing wound re-epithelialization
#21 Color because of perfusion by new capillary loops
Soft to touch, moist and granular in appearance
Granulation tissue begins to appear in human wounds by about day 4 post-injury
Initially consists of network of T-III collagen later replaced by stronger and long stranded type I collagen evidenced in scar tissue
#22 Granulation tissue fills the wound and keratinocytes migrate to restore epithelial continuity
Formation of actin filaments in the cytoplasm of keratinocytes, which provides them with the locomotion to actively migrate into the wound
Regression of the desmosomal connections between keratinocytes and to the underlying basement membrane frees cells and allows them to migrate laterally
Keratinocytes then move via interactions with ECM proteins (such as fibronectin, vitronectin, and type I collagen) via specific integrin mediators as they proceed between the desiccated eschar and the provisional fibrin matrix: beneath
#23 Fibroblasts are the workhorses during this time and produce the ECM that fills the healing scar and provides a scaffold for keratinocyte migration
Macrophages continue to produce growth factors such as PDGF and TGF-P1 that induce fibroblasts to proliferate, migrate, and deposit ECM, as well as stimulate endothelial cells to form new vessels.
#24 Angiogenesis is sprouting of capillaries from existing blood vessels in the wound edge tissue
Vasculogenesis – formation of new blood vessels by mobilization of bone marrow derived endothelial steam cells
During hemostasis, the hemostasis plug provides a bed to attract blood born cells to the wound
During inflammatory phase leukocytes serve as source of proangiogenic factors , VEGF & IL8
ECM molecules and ECM remodeling events play a key role in regulating angiogenesis
#25 The least understood phase of wound healing
Myofibroblasts are fibroblasts with intracellular actin microfilaments capable of force generation and matrix contraction
During inflammatory phase of wound healing fibroblasts acquire smooth muscle cell characteristics and differentiate into contractile myofibroblasts
#26 Type III collagen is initially laid down by fibroblasts during the proliferative phase, but over the next few weeks to months this will be replaced by type I collagen
#27 Need for nutrients such as carbohydrates, protiens, fat, aminoacids, vit and minirals
Malnutrition causes delayed neovascularization, dec. collagen synthesis, prolonged inflammation
Fats and carbohydrates provide primary energy source for collagen synthesis and angiogenesis; 30-35kcal/kg/day (nl adult) & 35-40kcal/kg/day (malnourished adult)
Proteins – fibroblast proliferation, collagen deposition, formation of vascular supply, immune response
0.8-1g/kg/day of protein is recommended for wound healing in normal adult 2g/kg/day for pts with chronic wounds
Vit A,C&E – antioxidant and anti inflammatory effect
#28 Is a defect in either regeneration or scar formation
Other examples of inadequate regeneration include bone nonunions and corneal ulcers
diabetic ulcers occur because of defects in the inflammatory and proliferative phases of wound healing
wounds occurring because of vitamin C depletion (i.e., scurvy) are due to abnormal collagen cross-linking, which occurs during the remodeling phase of wound healing
#29 In these situations, scar formation would be preferable to regeneration because of the risk of loss of growth control and possible transformation to overt cancer
Irritant strategies to maximize scar formation may also play a role, as when alcohol is injected into a neuroma
Therapeutic measures are targeted toward decreasing cellular proliferation and blocking the regenerative pathways or maximize scar formation
#30 Theories include mechanical strain, inflammation, bacterial colonization, and foreign body reaction
The prolonged secretion of inflammatory cytokines has been shown to induce fibrosis in numerous in vitro and animal models. Thus, researchers have long sought to manipulate the cytokine environment to prevent scar formation.
#31 <6% of the population (primarily blacks and Asians)
#33 Myoblasts join with each other to form myotubes which then fuse to form new myofibers.
Distructive, repair and remodeling
Initial neutrophil response followed by macrophages
#34 -lasting up to several weeks
-occurs concomitantly with repair phase
(to feed the upregulated metabolism of regeneration)
is necessary for functional regeneration
#35 (bypasses the stage of woven bone formation)
amount of callus correlates with the amount of instability encountered during healing
#36 Bone healing has 3 phases – inflammatory, reparative, remodeling
and tapering off when bone formation starts at 7 to 10 days
#37 (starting during the first week and lasting up to several months)
Acid tide—acidic local environment stimulates osteoclasts
PH rises at ~day 10 with the presence of increased alkaline phosphatase, leading to the
(starts a soft callus populated by chondrocytes, which gradually calcifies into hard callus by endochondral ossification); continued bone formation by osteoblasts leads to bony edge unification.
#38 (starting after fracture solidly united at 2 to 3 months and continuing for years)
(defined as the state of adequate stability and resolution of pain to allow protected motion)
#39 Intrinsic and extrinsic healing
(operative repair aims to maximize this type of healing)
#40 Immobilization* leads to the formation of debilitating adhesions to tendon limiting range of motion (early mobilization minimizes adhesions caused by extrinsic healing).
#41 Inflammatory, proliferating, remodeling
Starts within first few days, and peaks at 3 days
#42 starting at ~day 5 and lasting up to several weeks)
, proliferating from epitenon and endotenon
#43 (starting at several weeks after injury and lasting up to 1 year after)