Downloaded 99 times
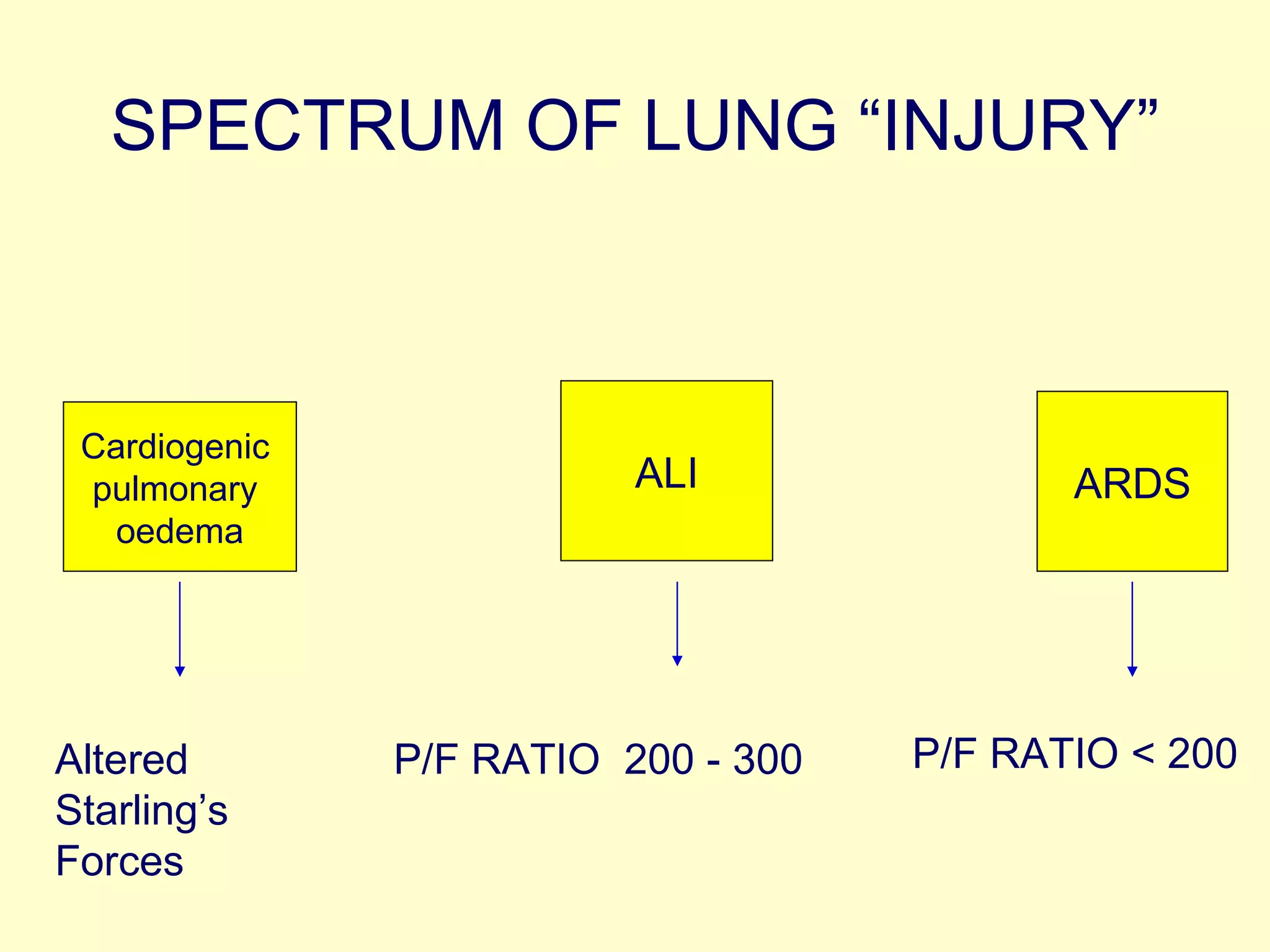


The document provides guidelines for the treatment of Acute Respiratory Distress Syndrome (ARDS). It discusses factors that cause ARDS and the spectrum of lung injury. Treatment guidelines cover oxygenation, ventilation, positioning, fluid management, and other modalities. Oxygenation goals aim to optimize oxygen levels while minimizing pressure and volume. Ventilation aims for low tidal volumes and pressures. Prone positioning may reduce mortality but did not consistently improve outcomes in studies. Conservative fluid management improved some outcomes compared to liberal management with no increase in complications.























































































