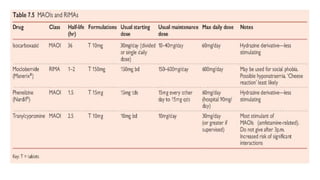
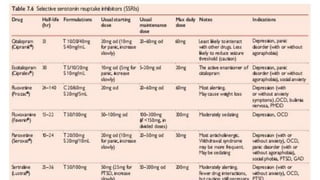
This document provides an overview of antidepressant medications. It begins with a brief history noting the accidental discovery of antidepressant effects from tuberculosis medications in the 1950s. It then covers the therapeutic uses and classifications of antidepressants, including tricyclic antidepressants, selective serotonin reuptake inhibitors, serotonin-norepinephrine reuptake inhibitors, and others. The mechanisms of action, uses, side effects, and drug interactions are described for different classes of antidepressants like monoamine oxidase inhibitors, tricyclics, and selective serotonin reuptake inhibitors.
![ANTIDEPRESSANTS
BY
UKPONG DISE-UTIBE P.
PSCHIATRY POSTING [M3]
UNIVERSITY OF UYO TEACHING HOSPITAL
JANUARY 2023](https://image.slidesharecdn.com/antidepressantsbydise-230509020439-2aee7623/85/Antidepressants-BY-Dise-pptx-1-320.jpg)
![ANTIDEPRESSANTS
BY
UKPONG DISE-UTIBE P.
PSCHIATRY POSTING [M3]
UNIVERSITY OF UYO TEACHING HOSPITAL
JANUARY 2023](https://image.slidesharecdn.com/antidepressantsbydise-230509020439-2aee7623/75/Antidepressants-BY-Dise-pptx-1-2048.jpg)
















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






