
Recommended
More Related Content
Similar to ANTIBACTERIAL DRUGS.pdfbbdbbdndbdnsjdbdjbdj
Similar to ANTIBACTERIAL DRUGS.pdfbbdbbdndbdnsjdbdjbdj (20)
More from Happychifunda
More from Happychifunda (20)
Recently uploaded
Recently uploaded (20)
ANTIBACTERIAL DRUGS.pdfbbdbbdndbdnsjdbdjbdj
- 1. ZERA INTERNATIONAL COLLEGE OF HEALTH SCIENCES CLINICAL MEDICINE DEPARTMENT. ANTI BACTERIAL DRUGS DR M KATASO MD.
- 2. GRAM –VE VS GRAM +VE 1. Gram +ve cells have a very thick, multilayered cell wall. Contain teichoic acids and lipoteichoic acid. 2. Gram -ve cells have a very thin layer of peptidoglycan. Have an outer (Lipid) membrane in addition to the cytoplasmic membrane, the space between these two membranes is called the periplasmic space or periplasm. • Clinical importance. 1. Gram +ve bacteria have highly porous membrane allowing large molecular weight and charged antibiotics to pass through and reach the binding sites. 2. Highly charged or large molecular weight antibiotics cannot cross the outer (lipid) membrane of the gram –ve bacteria to reach the binding sites in the inner cytoplasmic membrane
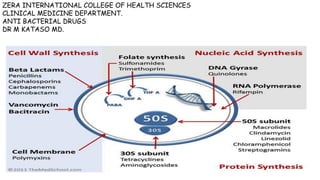
- 3. CLASSIFCATION BASED ON MOA
- 4. CELL WALL SYNTHESIS INHIBITORS 1. Cycloserine 2. Bacitracin 3. Vancomycin 4. Beta Lactams: listed below. I. Penicillin II. Cephalosporin's III.Carbapenems IV. Aztreonam
- 5. PENICILLINS • Contains one alterable side chain (R group), which can confer different antibacterial and pharmacological properties.
- 6. MECHANISM OF ACTION 1. Penicillin's inhibit bacterial cell wall synthesis by interfering with transpeptidation. 2. They bind to transpeptidase and act as competitive inhibitors leading to synthesis of a defective cell membrane, which is osmotically less stable. 3. Penicillin's are bactericidal (kill bacteria)
- 8. NATURAL PENICILIN/NARROW SPECTRUM BENZYL PENICILLIN (PENICILLIN G). 1. Greatest acvtivity against gram positive organisms like staph and strep. Also has activity againt Neisseria meningitides, clostridium tetanus, clostridium welchii, clostridium per-fringes, Neisseria gonorhoea, treponema pallidum and many other spirochetes, bacillus anthracis and other gram positive rods, listeria, actinomyces. 2. Inactivated by gastric acid therefore given IV or IM. PHENOXYMETHYL PENICILLIN (PENICILLIN V) 1. Stable to gastric acid therefore given orally less active than penicillin G. 2. Penicillin G and Penicillin V are inactivated by beta lactamases 3. Its given in minor infections because of its poor bioavailability 4 times dosing usually. ANTI-STAPHYLOCOCCAL 1. Penicillin resistant to beta-lactamases: Used for treatment of beta lactamase producing staphylococci infections 2. Very narrow spectrum 3. Examples: Methicillin, Nafcilllin, Cloxacillin, Dicloxacillin, Flucloxacillin, Oxacillin
- 9. CLINICAL USES OF NATURAL PENICILLINS Many are for streptococcal infections: 1. Oral pen V is the agent of choice group A streptococcal pharyngitis ( strep throat). 2. Pen V or G are treatments for Acute rheumatic fever due to group A streptococcal infection 3. Pen g treats left sided endocarditis caused by streptococcal viridans and streptococcal bovis 4. Intrapartum penicillin G is given as prophylaxis for group B streptococcus (strep agalactiae). 5. Single dose of penicillin G treats syphilis. ( treponema pallidum). 6. Pen G treats meningitis due to Neisseria meningitides. CLINICAL USES OF ANTI-STAPHYLOCOCCAL ANTI-BIOTICS. 1. Treats skin and soft tissue infections like folliculitis, abscess, carbuncle and furunacle. Gives as PO 2. Treats staphylococcal endocarditis 3. Treats staph osteomyelitis
- 10. BROAD SPECTRUM ANTIBIOTICS AMINO PENICILLINS 1. Members include: Ampicillin and Amoxicillin. 2. Amoxiccillin is good oral bioavalability. 3. Have more activity against gram -ve organisms than natural penicillins. 4. Easily inactivated by beta lactamases. 5. Ampicillin/Amoxicillin ‘HELPS’ to clear enterococci (Hemophylus influenza, E-coli, Listeria Monocytogens, Proteus and shigella). (‘Lipopolysacharides’). 6. Ampicillin and Amoxicillin can be protected from destruction by beta-lactamases if they are co-administered with beta lactamase inhibitors e.g. Amoxicillin + Clavulanic acid and Ampicillin + Sulbactam 7. Amoxicillin and Ampicillin are ineffective against pseudomonas. ANTIPSEUDOMONAL ANTIBIOTICS 1. Members include, Piperacillin, Ticarcillin, Carbenicillin, Azlocillin,Mezlocilin. 2. These can be protected from destruction by beta-lactamases if they are co-administered with beta lactamase inhibitors e.g.Piperacillin + Tazobactam, and Ticarcillin + Clavulanic acid. GENERAL ADVERSE EFFECTS FOR PENICILLINS 1. Hypersensitivity reactions and anaphylaxis (most dangerous). 2. Neurotoxicity with high doses 3. Nausea, diarrhea. 4. Antibiotic associated colitis (pseudomembranous colitis) with broad spectrum penicillins RESISTANCE 1. Acquired: Inactivation by Beta lactamases 2. Inherent: Penicillin Binding Protein (PBPs) located inside lipoprotein barrier.
- 11. CLINICAL USES OF AMINO-PENICILLINS ( AMOXICILLIN AND AMPICILLIN) 1. Treats streptococcal pharyngitis 2. Amoxicillin can also be used to treat otitis, sinusitis, and other respiratory illnesses caused by streptococcus pneumonia, hemophilus influenza and Moraxella catarhalis. 3. Amoxicillin is an option when treating pneumonia becauses of its activity against strep pneuminiae, hemophilus influenza, and Moraxella catarhalis. 4. Amoxicillin is part of the triple therapy for Helicobacter pylori in PUD. 5. Ampicillin is given as IV to treat serious anaerobic infections such as aspiration pneumonia. 6. Ampicillin treats enterococcus infections UTI and endocarditis. 7. Ampicillin can treat meningitis due to listeria monocytoges 8. Amoxicillin is used as chemoprophylaxis against encapsulated bacteria like strep pneumoniae, and hemophilus influenza in asplenic patients. 9. Amoxicillin is also used as chemoprophylaxis before dental procedure in patients at risk of endocarditis. CLINICAL USES OF ANTI-PSUEDOMONAL ANTI-BIOTICS 1. Treats anaerobic infections 2. Treats pseudomonal infections 3. Can be used in hospital acquired pneumonia 4. Can be used as empiric treatment for sepsis.
- 12. CEPHALOSPORINS • MECHANISM OF ACTION 1. Similar to penicillins: 2. Binding to specific penicillin binding proteins (PBPs) that serve as drug receptors on bacteria. 3. Inhibition of cell wall synthesis by blocking transpeptidation of peptidoglycan. 4. Activation of autolytic enzymes in the cell wall, which result in bacterial death.
- 13. CEPHALOSPORINS CLASSIFICATION OF CEPHALOSPORINS 1. Have been divided into the five major groups (generations) depending mainly on the spectrum of anti-microbial activity. 2. Broader spectrum of antibacterial activities 3. More stable/resistant to β-lactamase hydrolysis 4. All cephalosporin's are inactive against enterococci, Listeria and almost all against Methicillin-resistant staphylococci FIRST GENERATION CEPHALOSPORINS 1. Cephalexine, cefadroxil, cefazolin, cephaprin, cephalotin, caphadrin. 2. Active against G +ve and some G -ve 3. Uses: URTI, LRTI, UTI, Skin & soft tissue infections ( cellulitis), surgical prophylaxis. SECOND GENERATION CEPHALOSPORINS 1. Cefuroxime (IV), cefuroxime axetil (oral), cefoxitin, cefamandole, cefprozil 2. Have extended activity against GNB while retaining activity against G +ve orgs; 3. Cefoxitin and cefotaten have good activity against anaerobes 4. Uses: community acquired pneumonia, skin/soft tissue infections, URTI, mixed aerobic & anaerobic infections, surgical prophylaxis THIRD GENERATION CEPHALOSPORINS 1. Cefotaxime, ceftriazone, ceftazidime, cefpodoxime, cefixime, moxalactam, cefoperazone, and ceftizoxime 2. Extended G- activities but less G+ effects 3. Ceftazidime and cefoperazone have good activity against Pseudomonas spp 4. Ceftizoxime & moxalactam have good actively against bacteroides fragilis 5. Have longer t ½ so can be given once daily. 6. Uses: G- infections, pseudomonal infections, G- meningitis, gonorrhea, UTI, osteomyelitis 7. Not recommended for surgical prophylaxis
- 14. CLINICAL USES OF 1ST GENERATION CEPHALOSPORINS 1. Cellulitis and abscesses. 2. Strep pharyngitis 3. Can be used to treat UTI as it have activity against PECK: the UTI bugs (proteus, E coli and Kleibseilla) 4. Cephazolin is the drug of choice for surgical chemoprophylaxis CLI ICAL USES OF 3RD GENERATION CEPHALOSPORINS 1. Ceftriaxone or cefotaxime are used as empiric treatment for meningitis. Vancomycin may be added for extra gram positive coverage of resistant strep pneumonaie. For young and elderly patients Ampicillin may added to cover listeria monocytogens. 2. Treats community or hospital acquired pneumonia 3. Ceftazidime treats pseudomonal infections 4. Ceftriaxone treats endocarditis due to strep viridans and the HACEK organisms. 5. Ceftriaxone is used in empiric treatment of sepsis. 6. Single dose of IM ceftriaxone is the first line treatment for gonorrhea.
- 15. FOURTH GENERATION CEPHALOSPORINS 1. E.G.Cefepime 2. Broad spectrum. 3. More resistant to hydrolysis by β-lactamases 4. Good activity against Pseudomonas, enterobacteria, as well as Staph, Strept, haemophilus, and Neisseria 5. Uses: Infections caused by above organisms FITH GENERATION CEPHALOSPORINS 1. Ceftaroline, Ceftobiprole. Ceftaroline is broad spectrum with MRSA coverage. 2. Recently approved in USA 3. Active against MRSA, enterococci, and G- orgs 4. Good anti-pseudomonal activity 5. Increased binding to PBP 6. Clinical experience with the drugs is limited ADVERSE EFFECTS OF CEPHALOSPORINS 1. Local irritation after intramuscular injection 2. Thrombophlebitis after intravenous injection 3. Pseudomembranous colitis. 4. Allergic reactions: Similar to penicillin 5. Interstitial nephritis 6. Renal tubular necrosis 7. Bleeding disorders RESISTANCE 1. Inactivation by Beta lactamases 2. Alteration of Penicillin Binding Protein (PBP) 3. Decreased permeability of the bacteria cell that prevents the drug from reaching the PBP
- 16. OTHER BETA LACTAMS. A.MONOBACTAMS: AZTREONAM 1. Resistant to beta-lactamases and active against gram negative rods (including pseudomonas & serratia) 2. Have no activity against gram-positive bacteria or anaerobes B. CARBAPENEMS Examples: Imipenem, Meropenem. Have very broad spectrum of antimicrobial activity. Active against many aerobic & anaerobic gram-positive and gram-negative organisms. Pseudomonas rapidly develops resistance. Imipenem is used with Cilastatin that blocks its breakdown in the kidney. VANCOMYCIN 1. Vancomycin is active only against gram-positive microorganisms. 2. Acts by inhibiting cell wall synthesis. Inhibits biosynthesis of peptidoglycan. Peptidoglycan: Major structural component of bacterial cell wall CLINICAL USES 1. Used mainly against G(+) organisms e.g. Staph. epidermis, S.pyogenes, S.pneumonia 2. Drug of Choice for MRSA 3. Used to treat E. faecalis in combination with aminoglycosides in patients allergic to penicillin 4. No significant oral absorption, so given IV 5. Drug of choice for treating clostridium difficile colitis via oral administration ADVERSE EFFECTS: Nephrotoxicity, Pain and thrombophlebitis with IV route, Ototoxicity. Occasional mild hematuria, proteinuria, azotemia, casts in urine. Hypotensive reaction associated with rapid IV administration. Hypersensitivity-May occur in 5 to 10% of patients. Anaphylaxis, eosinophilia, drug fever, neutropenia
- 17. PROTEIN SYNRHESIS INHIBITORS Bacteriostatic Agents: 1. Tetracylines 2. Chloramphenicol 3. Macrolides, 4. Clindamycin 5. Linezolid Bactericidal Agents: 1. Aminoglycosides 2. Spectinomycin. 50s ribosome inhibitors 1. Macrolides 2. Chloraphenicol. 3. Linezolid. 30s ribosome inhibitors 1. Aminoglycosides 2. Tetracyclines.
- 18. TETRACYCLINES Specific drugs:Doxycycline, Minocycline, Tetracycline & Tigecycline Activity: Broad spectrum & Bacteriostatic Many G + and G – orgs, rickettsia, mycoplasma, and chlamydia Bacteria concentrate antibiotic internally. Has MRSA coverage CLASSIFICATION CLINICAL USES OF TETRACYCLINES Treatment of infections caused by 1. Mycoplasma: pneumonia and URTI. 2. Chlamydia : cervicitis, urethritis, PID 3. Spirochetes: Treponema pallidum – syphilis in penicillin allergic pts. 4. Zoonotic infections 5. Also used for Acne ADVERSE REACTIONS/SIDE EFFECTS 1. Tooth enamel dysplasia and possible reduction in bone growth in children.(avoid) 2. Impaired liver function during pregnancy.(avoid) 3. Sensitivity to light (photosensitivity) – Doxycycline 4. Superinfection leading to candidiasis or colitis 5. Fanconi syndrome for expired drugs. 6. Nausea, vomitinf and diarrhea. CONTRAINDICATIONS 1. Pregnancy 2. Children <8 yo 3. With antacids and foods rich in calcium, iron and magnesium Important pharmacokinetic info: 1. Excreted via feces: will not require dose adjustments in renal failure.
- 19. AMINOGLYCOSIDES They are bactericidal drugs. Examples include; Streptomycin, Kanamycin, Gentamicin, Tobramycin, Amikacin, and Neomycin (topical). Mostly are available in IV form as they have poor oral bioavailability Mode of action: They act by blocking bacterial protein synthesis by binding to the 30S ribosomal subunit. Antimicrobial activity: 1. Active against GN aerobic orgs and some GPs. 2. Many gram-negative and some gram-positive bacteria. 3. Amikacin, Gentamycin, Netimicin & Tobramycin are active against P. aeruginosa (GANT) 4. Not useful for anaerobic (oxygen required for uptake of antibiotic) or intracellular bacteria. 5. Synergy - The aminoglycosides synergize with beta-lactam antibiotics. The beta lactams inhibit cell wall synthesis and thereby increase the permeability of the aminoglycosides 6. Topical preparations (1-3 %) for eye infections Clinical Uses 1. Neomycin: remains active in GIT: used in bowel prep b4 colorectal surgery 2. Paromomycin: Active against entamoeba histolytica. 3. Gentamycin: systemic GN infections-septicemia, nosocomial RTI, complicated UTI & intra-abdominal surgery. 4. With penicillins to treat enterococcal endocarditis 5. Treatment of meningitis 6. Topical preparations for burns, wounds, eye infections, etc Adverse Effects 1. Nephrotoxicity; (Neomycin, Kanamicin, Amikacin) 2. Ototoxicity; Induces deafness (Neomycin, Tobramycin, Gentamycin) 3. Neuromuscular Blockade; Aminoglycosides can reduce the release of Ach from motor nerve terminals & cause neuromuscular blockade, leading to flaccid paralysis & respiratory failure
- 20. AMINOGLYCOSIDES RESISTANCE 1. Enzymatic inactivation by Bacteria 2. Alteration of Bacterial Binding site 3. Decreased uptake by bacteria 4. Aminoglycoside acetylation, adenylation. MACROLIDES Macrolide antibiotics have an antibacterial spectrum similar but not identical to that of penicillin. Examples: Erythromycin, Azithromycin, Roxithromycin Clarithromycin. Mechanism of action: Macrolides bind to bacterial 50S ribosomes and inhibit protein synthesis. General Activity 1. Broad spectrum of antimicrobial activity against: Gram positive cocci, Atypical organism (mycoplasma, chlamydia, Legionella pneumophilia, H.pylori- treatment of ulcers due to h.pylori, Treponema, Mycobacteriam avium General Clinical Uses 1. Community acquired pneumonia 2. Staphylococcal infections 3. Chlamydial infection: eyes, respiratory tract, genitals 4. Chemoprophylaxis against endocarditis resulting from dental procedures 5. Alternative for penicillin allergic patients 6. Clarithromycin is part of the triple therapy in PUD. 7. Erythromycin in neonatal conjuctivits
- 21. MACROLIDS ERYTHROMYCIN Spectrum; 1. Effective against Penicillin resistant Staph, S.pyogenes, S. viridans, S. pneumoniae, Anaerobic streptococci and many strains of S. faecalis 2. Also effective against Corynebacterium diphtheriae, Clostridia species, N gonorrhoea, Bordetella pertussis 3. Also sensitive are bacteroides, Mycoplasma pneumoniae, Treponema pallidum, Legionella pneumophila and many species of rickettsia & chlamydia. CLARYTHROMYCIN 1. 2 to 4 fold more active against streptococci & staphylococci 2. More active than erythromycin against pathogens responsible for atypical pneumoniaes: L. pneumophilia, Mycoplasma pneumoniae, Chlamydia pneumonia. AZITHROMYCIN 1. Unlike Erythromycin & Clarithromycin, it inhibits aerobic G-ve bacilli e.g. Enterobacteriaceae 2. Moderately active against salmonella, shigella, E. coli, Yersinia. 3. Excellent activity against Vibrio cholera, Gardenella vaginalis. ADVERSE EFFECTS 1. Erythromycin causes GI upset 2. Clarithromycin & Azithromycin better tolerated,. 3. Dose related hearing loss seen
- 22. CHLORAMPHENICOL 1. Broad spectrum antimicrobial and penetrates tissue very well. 2. It is bacteriostatic but bactericidal for H. Influenza; is extremely effective against streptococci and staphylococci. It is currently a backup drug for infections due to salmonella typhi, rickettsia and possibly in bacterial meningitis MoA: Inhibits 50S ribosomal subunit of bacteria Clinical Uses 1. Bacterial meningitis 2. Eye (Bacterial Conjunctivitis) and ear infections 3. Typhoid fever ADVERSE EFFECTS 1. Nausea, vomiting and diarrhea 2. Predispose to Candida infections (oral and vaginal) 3. Dose related myelosuppression (Aplastic anemia) 4. In babies due to inadequate metabolism & excretion can result in ‘grey baby syndrome’ . LINEZOLID Broad spectrum bacteriostatic antibacterial Activity includes Staph, Strept, enterococci, mycobacteria Uses: Community Acquired Bacterial Pneumonia (CABP), HABP, skin and soft tissue infections A/E: marrow suppression, neuropathy, serotonin syndrome if used with SSRI
- 23. NUCLEIC ACID SYNTHESIS INHIBITORS THE FOLLOWING DRUGS CAN INTERFFERE WITH DNA OR RNA SYNTHESIS 1. ANTIFOLATE/ANTIMETABOLITES/SULFONAMIDES 2. QUINOLONES 3. METRONIDAZOLE 4. RIFAMYCINS.
- 24. NUCLEIC ACID SYNTHESIS INHIBITORS ANTI-METABOLITES SULFONAMIDES AND TRIMETHOPRIM They inhibit the enzymes required in the synthesis of DNA. The reaction below shows a summarized enzymatic steps involved in DNA synthesis of bacteria. Key: PABA: para-amino bemzoic acid DHF: dihydrofolate THF: tetrahydrofolate Purine: monomer for DNA. DNA: deoxyribonucleic acid A = Dihydropteroate synthase (inhibited by sulfonamides) B = Dihydrofolate reductase (inhibited by trimethoprim and pyrimethamine). SULFONAMIDES 1. Sulfadiazine: Short acting: (4-8 hrs) 2. Sulfamethoxazole: Intermediate acting (8-12hrs) 3. Sulfadoxine: Long acting: (7 days) 4. Sulfacetamide: 5. Sulfasalazin 1. Combination of ‘A’ inhibitor and ‘B’ inhibitor as above produces synergism.
- 25. SULFONAMIDES 1. The drugs are also called Anti folate. 2. Resistance develops readily on monotherapy so combination with trimethoprim or pyrimethamine often used. The Combination produces synergism. 3. Sulfonamides and trimethoprim (or pyrimethamine) are often formulated in fixed dose combinations. 4. Alone drugs are bacteriostatic, in combination they are bactericidal. 5. Active against G-ve and G+ve orgs, chlamydia and protozoa. Has activity against MRSA. CLINICAL USES: A. TRIMETHOPRIM SULFAMETHOXAZOLE (A.K.A- Cotrimoxazole, Bactrim or septrin or septra). 1. First line treatment for UTI: Cystitis, prostatitis. 2. Treatment of pneumocystis jiroveci pneumonia (PJP). 3. Used as chemoprophylaxis againt PJP in HIV infected patients with CD4 count <200 4. Used as chemoprophylaxis against Toxoplasmosis in HIV infected patients with CD4 count < 100. 5. Can treat infection of GIT and Respiratory infection caused by gram positive and gram negative bacteria. B. PYRIMETHAMINE SULFADIAZINE: 1. Treats Toxoplasmosis caused by Toxoplasma Gondi. C. SULFADOXINE/PYRIMETHAMINE (A.K.A fansidar) 1. Treats malaria 2. Used as chemoprophylaxis against Malaria in pregnant women. D. SULFASALAZINE: not absorbed orally) Used for ulcerative colitis and inflammatory bowel diseases E. SULFACETAMIDE: available as topical preparation for eye infections (chlamydia).
- 26. CONTRAINDICATIONS 1. Severe allergy to sulfa drugs 2. First trimester pregnancy 3. Severe renal insufficiency (Cr>1.5mg/dl) 4. Severe hepatic disease 5. pancytopenia ADVERSE REACTIONS 1. Allergic reactions: Skin rash, fever, dermatitis, stomatitis, urticarial 2. Urinary tract obstruction, nephritis 3. Hemolytic anemia in G6PD deficiency; aplastic anemia 4. Kernicterus if given in the last month of pregnancy 5. CYP 450 inhibitor: drug to drug interactions. 6. Megaloblastic anemia, bone marrow suppression 7. GI related disturbances 8. Renal failure.
- 27. TOPOISOMERASE INHIBITORS The drugs include quinolones and Fluoroquinolones. Inhibition of topoisomerases II (DNA gyrase) and prevents replication or transcription of DNA. Inhibition of topoisomerase IV halts separation of replicated chromosomes into daughter cells. Topoisomerase inhibitors inhibit both enzymes A. QUINOLONES Have quinolone structure Active primarily against G -ve bacteria 1. NALIDIXIC ACID • Bactericidal • Active against E. coli, Proteus, Klebsiella, Enterobacter, Shigella but not Pseudomonas • Used primarily for urinary antiseptic • Also for diarrhea caused by Proteus, Shigella, Salmonella • Resistance develops rapidly. B. FLUOROQUINOLONES There are 4 importanta generations of fluoroquinolones.
- 28. The table below shows the generations, examples and the spectrum of activity. CIPROFLOXACIN Used for the treatment of: 1. Acute bronchitis, acute pneumonia, 2. UTI, skin 3. Soft tissue infection Bone & joint infection 4. Bacterial gastroenteritis 5. Typhoid. GENERATIONS DRUGS SPECTRUM 1ST NALIDIXIC ACID G-VE But not pseudomonas 2nd Ciprofloxacin Norfloxacin Enoxacin ofloxacin G –VE including pseudomonas, some G+VE & atypicals 3rd Levofloxacin Sparfloxacin gemifloxacin Same as 2nd generation with extended G+ve & atypical coverage 4th Moxifloxacin trovafloxacin Same as third with broad anaerobic coverage. 6. Tuberculosis: Used as a component of combination chemotherapy against multidrug resistant tuberculosis 7. G –ve meningitis in immunocompromised patients or those with CSF shunts 8. Topical therapy for G-ve conjunctivitis 3rd and 4th generation are reffered to as respiratory fluoroquinolones.
- 29. CONTRAINDICATIONS 1. Children < 18 yo 2. Pregnancy 3. Lactating women. ADVERSE EFFECTS 1. GIT related Upsets 2. ECG abnormalities : arrhythmias 3. Destruction of cartilage in growing children –arthropathy 4. Tendonitis (adults).
- 30. METRONIDAZOLE MECHANISM OF ACTION. Its nitro group is reduced by certain redox proteins operative only in anaerobic bacteria to highly reactive nitro radical which exerts cytotoxicity. This leads to disruption of energy metabolism of anaerobes by hindering the replication, transcription & repair process of DNA resulting in cell death. Presence of oxygen prevents reduction of metronidazole & so reduces its cytotoxicity. ACTIVITY Good coverage for anaerobic bactria Has antiparasitic activity: trichomoniasis, Giardia lambria, amoeba etc. USES GI infections caused by the above mentioned microbes (below the diaphragm) ADVERSE EFFECTS Anorexia, nausea, metallic taste, abdominal cramps Prolonged administration may cause peripheral neuropathy & CNS effects. Seizures with high doses Thrombophlebitis of the injected vein if solution is not well diluted
- 31. RIFAMYCINS 1. Interffere with transcription of DNA into RNA inhibiting RNA polymerase. 2. Examples include: rifampin, rifabutin & rifampentine. THE DRUGS WILL BE DISCUSSED SEPERATELY IN ATITUBERCULOUS DRUS ( ANTI- TB DRUGS). THE END THANK YOU FOR YOUR ATTENTION