Download as PDF, PPTX


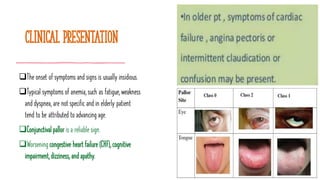

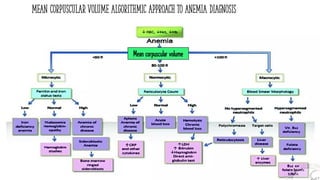
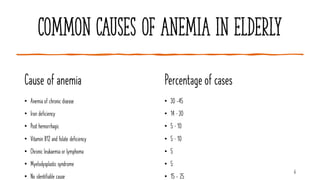




Anemia in the elderly is characterized by low hemoglobin levels and is prevalent in 8 to 44 percent of this population, often linked to underlying conditions rather than aging itself. Common causes include chronic disease, iron deficiencies, and vitamin B12 deficiencies, each requiring specific evaluation and treatment approaches. Effective management focuses on addressing the underlying causes and ensuring nutritional adequacy, alongside careful monitoring of symptoms and laboratory values.




















































































