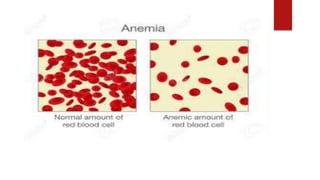
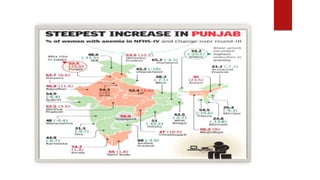
Anemia is a serious medical condition characterized by insufficient healthy red blood cells, affecting a significant portion of the global population, particularly in India where it impacts 50% of the population and leads to complications in women and children. Various types of anemia exist, such as iron-deficiency anemia and pernicious anemia, with multiple causes including dietary deficiencies, chronic illnesses, and pregnancy-related factors. Treatment and prevention strategies include dietary modifications, iron supplementation, education about nutritional needs, and food fortification measures.