The document provides an overview of intraoral scanners, detailing their technology, components, benefits, and various models available in the market. It explains the principles behind image acquisition and factors affecting scanning accuracy, while also presenting comparative analysis results on scan performance. The conclusion emphasizes the importance of modern intraoral scanners in enhancing dental workflows and patient experience.








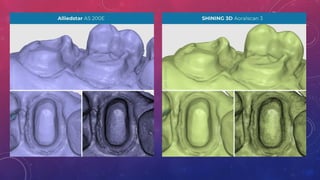
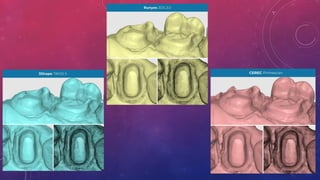
![• Across all the evaluated digital intraoral scanners, TRIOS 5 emerged as
the ,most accurate ]in recording data.
• Moreover, the output of all four scanners falls within a clinically
acceptable range for full arch digital impression utility.](https://image.slidesharecdn.com/aninsightintointraoralscanner-241019132430-d57080f2/85/An-insight-into-intraoral-scanner-technology-26-320.jpg)



































































![Certificate of Appreciation[1].pptx2222222222](https://cdn.slidesharecdn.com/ss_thumbnails/certificateofappreciation1-250126065929-9fa4e5b9-thumbnail.jpg?width=640&height=640&fit=bounds)




![An Alternative Technique For Transferring Ala‑tragus[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/analternativetechniquefortransferringalatragus1-241212212559-690c41e9-thumbnail.jpg?width=640&height=640&fit=bounds)






















