Download to read offline

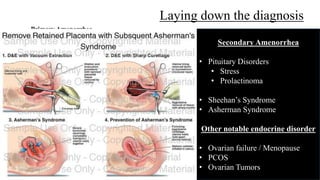
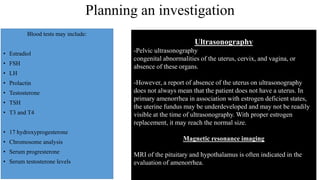

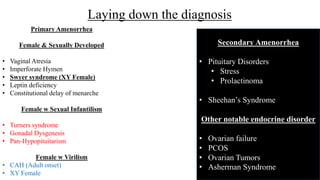

This document discusses the evaluation and diagnosis of a 17-year-old girl presenting with absence of menses (amenorrhea). It provides a list of potential causes to consider and evaluate through history, physical exam, and testing, including pregnancy, medical conditions, and endocrine or anatomical abnormalities. If diagnosis is secondary amenorrhea, potential causes include pituitary disorders, stress, prolactinoma, Sheehan's syndrome, or ovarian failure; if primary amenorrhea, causes may include vaginal atresia, imperforate hymen, Turner syndrome, or other intersex conditions. Laboratory tests and imaging can help identify the specific diagnosis.