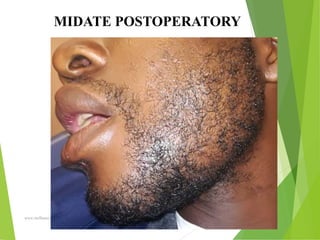
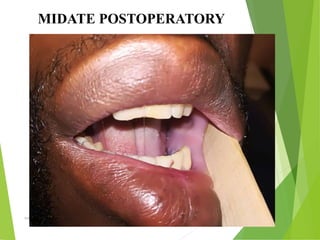
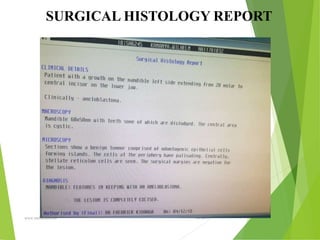
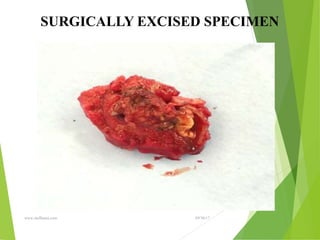
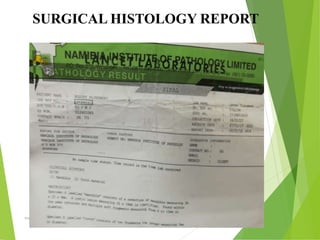
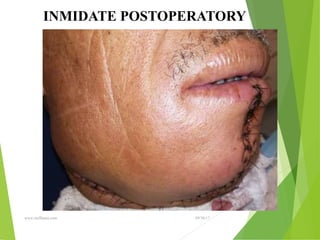
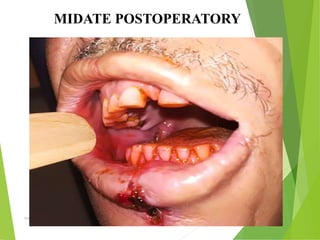
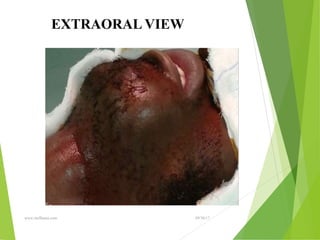
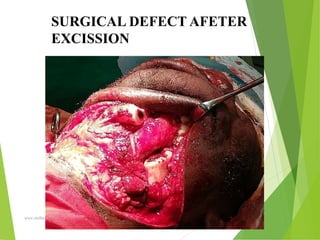
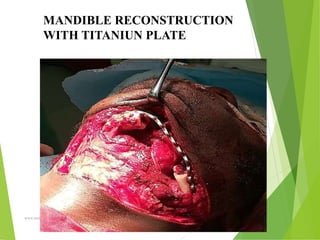
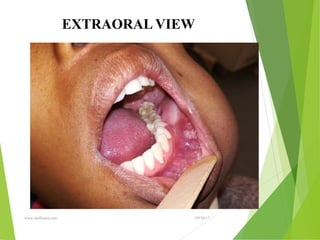
This document presents a case study of ameloblastoma, a benign odontogenic tumor. It defines ameloblastoma, discusses its epidemiology and classifications. The document describes the clinical features, radiological findings, differential diagnosis, management and prognosis of ameloblastoma. It then presents clinical case examples, including details of patients' examinations, radiographs, surgical procedures and histopathology reports. The conclusion emphasizes the need for long-term follow-up due to the high recurrence rate of ameloblastoma.

















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















