Downloaded 25 times
![Reporting that more
businesses are
showing interest in
preventive medicine
programs, this feature
targets physicians who
might take advantage
of the trend by sharing
the experiences of
those who are doing it
now. To accompany
another useful graphic,
which outlines how
to make a wellness
program work, this paired data graphic is an
important jump-page device to entice skimming
readers into the story. By delivering simple
comparisons in a familiar advantage/disadvan-
tage format, the graphic acts as a box score.
Interested readers will turn to the story for more
information while those who have read the story
will have a handy reminder of the business
models discussed.
PAGE 5
FOCUS ON PREVENTIVE MEDICINE
Wellness programs come in many shapes and sizes, presenting a wide array of business
opportunities for physicians. Here are descriptions of a few models:
Contracted services
An individual
physician offers services
to a hospital that has
created a wellness
clinic.
You can tailor your own offerings
and develop your practice accord-
ing to how many wellness patients
you want to see.
The partnering company handles
marketing, billing and other
services geared to get the wellness
business off the ground.
You can maintain your own prac-
tice while working with wellness
patients for a few hours each week.
You also don’t have to worry about
marketing the business.
You have to do your own sales
and marketing.
Your schedule is subject to
how busy the wellness clinic
becomes, and you don’t have as
much control as you would if
you ran the clinic yourself.
You have less control over
clinic operations and have to
pay a management fee. You may
not have the space necessary to
accommodate a partnership
clinic, or you might have to
renovate your current space.
Partnership with a
management
company
Developing business-
es offers turnkey
services to physicians
and hospitals for a
management fee.
ADVANTAGESMODEL DISADVANTAGES
Wellness practice
A physician group
offers wellness services
to local businesses.
1
Can we show
meaningful
comparisons?
F
or an afternoon every week
or two, internist Richard Hilde-
brand, MD, practices medicine in
a way that would make most physi-
cians jealous.
As medical director at the Center
for Preventive Medicine, part of St.
Luke’s Health System in Sioux City,
Iowa, Dr. Hildebrand spends two or
three hours with the same patient. He
focuses not on acute illnesses, but on
wellness. He puts the patient through
a series of tests, and actually has time
to go over results with him or her
once they’re completed.
“Over time — and I hate to speak
for everybody — we’ve gotten used to
the appointments every 10 or 20 min-
utes,” Dr. Hildebrand said. “This is a
nice combination of very old-fash-
ioned, but very high-tech. It makes a
lot of sense.”
Employers think so, too. More com-
panies are joining in the wellness
trend, sponsoring pre-
ventive health pro-
grams and asking — or,
in some cases, requir-
ing — their employees
to enroll. Programs
range from one-dimen-
sional, single-issue pro-
grams such as smoking cessation to di-
verse, multipurpose strategies that
look at a person’s overall health.
Sensing a business opportunity,
some physicians are starting to adapt
their practices to fit this trend as well.
Some are providing contracted ser-
vices to hospitals, while others are tai-
loring wellness programs and market-
ing them directly to local businesses.
A few doctors even are partnering
with fledgling businesses providing
turnkey-style support or other ser-
vices to help them get their wellness
practices off the ground.
Regardless of the size of the busi-
ness or practice, they have a straight-
forward sales pitch to employers:
wellness programs will save busi-
nesses money.
“It saves on insurance costs, and
we’ve seen amazing successes in sav-
ing people’s jobs from things like ad-
dictions, surgeries and life stresses,”
said Lee Rice, DO, a family physician
and sports medicine specialist in San
Diego. Dr. Rice is also CEO and med-
ical director of Lifewellness Institute,
a preventive medicine practice. “Busi-
nesses see employees as their most im-
portant asset, and they want their em-
ployees to know it,” Dr. Rice said.
Employers see corporate wellness
programs as a way to both control
health care costs and boost key em-
ployees’ productivity. The theory is a
AMERICAN MEDICAL NEWS AMEDNEWS.COM JUNE 5, 2006
17
BusinessPRACTICE MANAGEMENT n PERSONAL FINANCE n TECHNOLOGY
Physicians score victory in class-action compliance settlement [ PAGE 19 ]
Businesses are
showing more
interest in
preventive medicine
programs, providing
a new business
opportunity for
physicians.
Wellnessgoes to
work
MAKING
WELLNESS
WORK
A 2005 Hewitt Associates
survey says employers
are developing more of
an interest in corporate
wellness programs. Here
are some reasons why:
n Insurance expenses are
rising.
n Healthy employees are
more productive and
miss less work time.
n It’s a cost-effective way
to prove to employees
that the company cares
for their well-being.
Here are some condi-
tions that can make
wellness programs a
good business opportuni-
ty for physicians:
POPULATION
More densely populated
areas could provide a
large enough pool of
people interested in
wellness.
NUMBER OF BUSINESSES
The more corporate
clients you can sign up,
the greater percentage
of your practice you
dedicate to wellness.
TYPES OF BUSINESSES
Large manufacturing
facilities might not find
all-inclusive programs to
be cost-effective, but they
could contract for single
services, such as nutri-
tional counseling or
tobacco cessation. Small,
self-insured, white-collar
businesses, meanwhile,
may be interested in
comprehensive care.
CONTACT WITH DECISION
MAKERS
If you belong to a local
club or know local busi-
ness CEOs through work
or business circles, you
might have a better
chance of marketing
your wellness services
and landing corporate
clients.
Continued on next page
Richard Hildebrand, MD
Story by
Mike Norbut
Photo by
Greg Latza](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-5-320.jpg)
![n Allows physicians to spot areas that need improvement and lets
them use the knowledge to make changes.
n Lets payers reward physicians who perform better with more
referrals and bonus pay.
n Empowers consumers to choose physicians on the basis of both
quality and cost, particularly with the number of patients using
health savings accounts at 3.2 million and growing. Increased
competition for patients will lead to overall quality improvement.
n Quality measurement can be inaccurate if it is based on admin-
istrative claims data that do not capture the entirety of a patient’s
circumstances.
n Compliance can be costly. Either a practice must do timely,
expensive chart reviews or spend heavily on electronic medical
record systems.
n Quality measures can unfairly represent physicians’
performance. For example, outcome-based measures can penalize
physicians who see patients who are sicker or face economic,
cultural and linguistic barriers to complying with doctors’ orders.
n When paired with pay-for-performance, quality measurement
could merely reward larger practices that have made costly
technology investments and practices in higher-income areas.
Perversely, quality measurement could divert resources away
from already underserved areas.
PAGE 6
ASSESSING QUALITY
The era of measuring physician performance is likely here to
stay. Drawn from a range of perspectives, experts say these are
some of the pros and cons of quality measurement.
PROS
CONS
The headline sums up this story well: Quality quandary.
Performance measures have doctors up in arms. Some
physicians can see benefits if it is done right. Other physicians
say the entire idea is flawed. The story focuses on the issue of
physicians being worried that quality measures could leave
behind the sickest and most vulnerable patients because
doctors don’t want to be dinged on quality measures for
patients they know won’t improve. The pro/con box that
accompanies the story takes a bigger look at the pay-for-
performance issue and sums up doctors’ likes and dislikes
about being assessed for quality.
It sums up concerns in many areas,
not just the issue of patient care.
1
Can we show
meaningful
comparisons?
MAY 22/29, 2006 AMEDNEWS.COM AMERICAN MEDICAL NEWS
12
Professional Issues
FSMB data show modest dip in disciplinary actions [ PAGE 15 ]
HEALTH CARE LITIGATION n MEDICAL EDUCATION n ETHICS n PROFESSIONAL REGULATION
C
an a number tell the world how good a doctor is? A lot
of people are counting on it. The government, health
plans and employers are demanding a way to quantify
the value they’re getting for their health care dollars.
Patients, faced with higher co-pays and deductibles and
increasingly invested in health savings accounts, want
reliable public ratings of doctors’ performance.
Only a third of physicians have access to any data about
their own clinical performance, and just a quarter have
the electronic medical records systems considered essen-
tial for continuous quality improvement, according to a
2003 Commonwealth Fund survey of doctors. Still, a small
but growing number of physicians who have assessed the
quality of care they deliver as part of maintenance-of-certi-
fication and pay-for-performance programs see quality
measurement as helpful to care better for their patients.
But many physicians, embittered by early and clumsy
attempts by outsiders to gauge their performance, have
deep concerns about the accuracy and fairness of quality
measurement. With more than 100 pay-for-performance
programs up and running, according to the Leapfrog
Group, and the Centers for Medicare & Medicaid Services
asking physicians to voluntarily report quality data, it
seems quality measurement is here to stay.
Yet as physician groups take over the reins in develop-
ing quality measures for payers and the public to use, a
quandary presents itself: Could attempts to improve quality
by measuring it have the perverse effect of punishing doc-
tors who care for the most vulnerable patient populations?
Skeptical doctors say the medical experts, academicians,
methodologists and statisticians charged with developing
quality measures must be mindful of their potential impact
on practicing physicians and the patients they serve.
Concerns about patient outcomes
R
andall Maxey, MD, PhD, approves of the quality mea-
surement idea in general but worries about whether
its use could wind up penalizing physicians who prac-
tice in underserved areas. While most measures gauge
how often physicians deliver clinically recommended
care, a few very important ones hold doctors accountable
for their patients’ outcomes.
“It’s going to be a lot easier to treat a little old lady from
Beverly Hills,” said Dr. Maxey, an Inglewood, Calif.,
nephrologist who co-chairs the Commission to End Health
Care Disparities and a National Medical Assn. former
president. “Some communities are more compliant and
more health-literate and have more resources to influence
outcomes than others. I may treat you exactly correctly
and give you the right pills, but if you have to choose be-
tween buying pills and giving your baby milk, that drug
may lose out and my performance may be judged as poor
because of it.”
Roy M. Poses, MD, shares Dr. Maxey’s concern.
Qquandary
Quality
PHOTO©JOHNFORASTÉ
ASSESSING
QUALITY
The era of measuring physi-
cian performance is likely
here to stay. Drawn from
a range of perspectives,
experts say these are some of
the pros and cons of quality
measurement.
PROS
n Allows physicians to spot
areas that need improvement
and lets them use the
knowledge to make changes.
n Lets payers reward
physicians who perform
better with more referrals
and bonus pay.
n Empowers consumers to
choose physicians on the
basis of both quality and
cost, particularly with the
number of patients using
health savings accounts at
3.2 million and growing.
Increased competition for
patients will lead to overall
quality improvement.
n Quality measurement can
be inaccurate if it is based on
administrative claims data
that do not capture the
entirety of a patient’s
circumstances.
n Compliance can be costly.
Either a practice must do
timely, expensive chart
reviews or spend heavily on
electronic medical record
systems.
n Quality measures can
unfairly represent
physicians’ performance.
For example, outcome-based
measures can penalize
physicians who see patients
who are sicker or face
economic, cultural and
linguistic barriers to
complying with doctors’
orders.
n When paired with pay-
for-performance, quality
measurement could merely
reward larger practices that
have made costly technology
investments and practices
in higher-income areas.
Perversely, quality measure-
ment could divert resources
away from already under-
served areas.
CONS
As the movement to
measure quality forges
ahead, some physicians
worry their patients
could be left behind.
Story by Kevin B. O’Reilly
Outcome-based measurements need to control for patient characteristics, said internist Roy M. Poses, MD.](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-6-320.jpg)
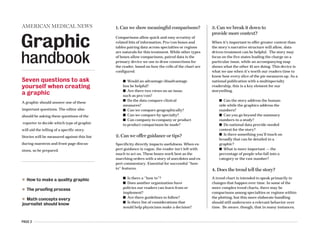
![PAGE 7
To bring greater clarity to a story
about the link between quality and
volume in nonsurgical care, this
graphic presented valuable data for
comparison. It is based on a study of
pneumonia patients, and in a simple
manner, lays out key findings for
four levels of patient volume. A few
key findings are explained to set up
the top of the story, but it’s the
graphic that carries the essential
details.
1
Can we show
meaningful
comparisons?
n Doctors say the decision
opens the door for “junk
science.”
AMY LYNN SORREL
AMNEWS STAFF
If a New York appeals court ruling
that loosened rules for expert witness
testimony allowed in medical liability
cases stands, physicians say it will
open the gate for unreliable scientific
evidence to enter the courtroom.
In a unanimous opinion, the Appel-
late Division of the Supreme Court,
the state’s intermediate level, said ex-
perts did not need to show peer-re-
viewed medical literature to prove
that their medical opinion was accept-
ed in the scientific community.
Judges found that a lower court ap-
plied the testimony rule “too restric-
tively” when it wouldn’t allow the tes-
timony and dismissed the case.
Physicians say the appeals court
ruling defies state precedent uphold-
ing rigorous scrutiny of what testimo-
ny is permitted to be heard by jurors.
If the courts don’t adhere to the stan-
dard, physicians say, ripple effects
could cause meritless lawsuits to en-
ter the legal system.
Lawyers for the physician in the
case are asking the appeals court to
reconsider. If that doesn’t happen,
they will ask the state’s high court to
overturn the ruling. The medical com-
munity has weighed in on the physi-
cian’s side, with doctors and a phar-
maceutical company fearing that the
ruling would be used as an example
for other courts to relax the rule if it’s
not reversed.
“There should be a high standard,
and it’s up to the courts to make sure
that any medical theory being [pre-
sented] actually has the support of the
profession,” said Donald Moy, general
counsel to the Medical Society of the
State of New York, which filed a
friend-of-the-court brief with the
American Medical Association and
Pfizer. The company didn’t manufac-
ture the drug in the lawsuit but does
not want to see a precedent set.
Allowing only peer-reviewed liter-
ature is critical, Moy explained, be-
cause it is often difficult for a jury to
differentiate between credible science
and “junk science.”
Mary Beth Ott, who represents the
plaintiff, said the appeals court ruling
is correct, “and that’s the law as it
stands now.” Ott declined to comment
further, citing the pending litigation.
Did a drug trigger a disease?
The case, Zito v. Zabarsky, stems from
a November 2003 trial court hearing
to screen expert witness testimony.
New York courts require the testimo-
ny with the plaintiff’s filing of a med-
ical liability case to determine the va-
lidity of claims made. Judges follow
the Frye standard, derived from a 1923
federal ruling that established that
novel scientific evidence presented in
court must “have gained general ac-
ceptance” in the relevant scientific
community.
Pamela Zito sued Queens internist
Gary Zabarsky, MD, alleging that he
had prescribed her an “excessive”
dose of the cholesterol drug, Zocor
(simvastatin), which caused her to de-
velop an autoimmune disease, court
records show. Dr. Zabarsky denies the
n For diseases such as pneumonia, higher
patient volume could mean worse
physician performance.
KEVIN B. O’REILLY
AMNEWS STAFF
Practice makes perfect? Not always. That’s the find-
ing of a recent study that sought to find out whether
physicians who cared for a higher volume of pneu-
monia patients in a given year were more likely
to follow quality guidelines and achieve superior
outcomes.
Hundreds of studies have used patient volume as
a proxy in quality measurement for high-risk surgi-
cal procedures, such as coronary bypass artery
graft or care for complex diseases such as
HIV/AIDS. Nearly 70% of studies examining physi-
cian performance in those areas found a statistical-
ly significant association between higher patient
volume and superior outcomes, according to a 2002
medical literature review published in the Annals
of Internal Medicine.
But the much-touted volume-outcome correla-
tion appears to fall apart for care such as pneumo-
nia, according to a study published in the Feb. 21
Annals of Internal Medicine.
The evaluation of 9,741 doctors who cared for
AMERICAN MEDICAL NEWS AMEDNEWS.COM MAY 1, 2006
11
Professional IssuesHEALTH CARE LITIGATION n MEDICAL EDUCATION n ETHICS n PROFESSIONAL REGULATION
ETHICS FORUM: Apply standards of care equitably [ PAGE 16 ]
Volume-quality correlation
not clear cut, study says
Continued on page 14
Court lowers bar on scientific evidence
CASE AT A GLANCE
Pamela Zito v. Gary Zabarsky, MD
Venue: New York Supreme
Court, Appellate Division,
Second Department
At issue: Whether medical
expert testimony required in
medical liability cases must
include peer-reviewed literature
to show that an opinion is
generally accepted by the
scientific community. The
appeals court said no.
Potential impact: Physicians
say the ruling goes against
precedent, exposing doctors to
more lawsuits. The court said a
high standard deprives injured
plaintiffs of their day in court.
Continued on next page
New York appeals court ruling
“It’s up to the courts to
make sure any medical
theory ... has support of
the profession.”
Donald Moy, MSSNY general counsel
DISCOUNTING VOLUME
Hundreds of studies have found that for complicated surgeries and medical care such as coronary
artery bypass grafting or HIV/AIDS care, the higher the volume of cases a physician or hospital sees,
the better the outcomes. But for care such as pneumonia, the relationship between the volume of cas-
es and physician performance isn’t so clear, according to a recent study of 9,741
doctors who cared for 13,480 patients admitted to hospitals for pneumonia. The study’s authors broke
physicians into four groups based on the volume of pneumonia patients they cared for over a year.
Here are some of the results:
Study groups: 1 2 3 4
Median annual pneumonia cases 4 9 15 29
per physician
Percentage of time task performed
First antibiotic administered less 59% 63% 62% 62%
than four hours after admission
Appropriate antibiotics 82% 81% 81% 79%
Blood cultures obtained before 84% 84% 84% 83%
administration of antibiotics
Screened for or given influenza vaccine 21% 19% 20% 12%
Screened for or given pneumococcal vaccine 16% 13% 13% 9%
Results
Mean length of stay (in days) 6.0 6.0 6.2 6.6
Percentage of patients who died 5.8% 6.0% 5.7% 6.6%
in the hospital
Percentage of patients who died 10.9% 11.8% 11.0% 12.5%
within 30 days
SOURCE: “VOLUME, QUALITY OF CARE, AND OUTCOME IN PNEUMONIA,” ANNALS OF INTERNAL MEDICINE, FEB. 21
VOLUME
OF CASES
QUALITY
INDICATOR
OUTCOMES
DISCOUNTING VOLUME
Hundreds of studies have found that for complicated surgeries and medical care such as coronary
artery bypass grafting or HIV/AIDS care, the higher the volume of cases a physician or hospital sees,
the better the outcomes. But for care such as pneumonia, the relationship between the volume of
cases and physician performance isn’t so clear, according to a recent study of 9,741 doctors who
cared for 13,480 patients admitted to hospitals for pneumonia. The study’s authors broke physicians
into four groups based on the volume of pneumonia patients they cared for over a year. Here are
some of the results:
Study groups: 1 2 3 4
Median annual pneumonia cases 4 9 15 29
per physician
Percentage of time task performed
First antibiotic administered less 59% 63% 62% 62%
than four hours after admission
Appropriate antibiotics 82% 81% 81% 79%
Blood cultures obtained before 84% 84% 84% 83%
administration of antibiotics
Screened for or given influenza vaccine 21% 19% 20% 12%
Screened for or given pneumococcal vaccine 16% 13% 13% 9%
Results
Mean length of stay (in days) 6.0 6.0 6.2 6.6
Percentage of patients who died 5.8% 6.0% 5.7% 6.6%
in the hospital
Percentage of patients who died 10.9% 11.8% 11.0% 12.5%
within 30 days
SOURCE: “VOLUME, QUALITY OF CARE, AND OUTCOME IN PNEUMONIA,” ANNALS OF INTERNAL MEDICINE, FEB. 21
VOLUME
OF CASES
QUALITY
INDICATOR
OUTCOMES](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-7-320.jpg)
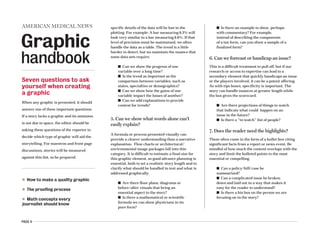
![PAGE 8
Heart disease kills more women than
any other disease. This story focuses
on the fact that other diseases are
better screened and looks at which
women are at the highest risk for
heart disease. The graphic shows the
five leading causes of death for
women and gives context for the
story. Easy comparison is drawn from
the plotting to emphasize just how
many more women die from
cardiovascular-related issues than
from the second leading cause,
cancer. By including factoids on
cardiovascular disease, the graphic
teases out more statistics about how
women are impacted.
1
Can we show
meaningful
comparisons?
SOURCE: CENTERS FOR DISEASE CONTROL AND PREVENTION AND
THE NATIONAL HEART, LUNG AND BLOOD INSTITUTE
n Cardiovascular disease (CVD)
ranks first among all disease
categories in hospital dis-
charges for women.
n Of the approximately 5.5
million stroke survivors alive
today, 56% are women.
n Misperceptions still exist that
CVD is not a real problem for
women.
n CVD is a particularly
important problem among mi-
nority women; the death rate
due to CVD is higher in black
women than in white women.
n 38% of women compared with
25% of men will die within one
year after a heart attack.
SOURCE: AMERICAN HEART ASSN.
Cardiovascular death: 484,000
Alzheimer’s
disease: 45,000
Diabetes
mellitus: 39,000
LEADING CAUSES OF DEATH FOR WOMEN
in the United States, 2003
Cancer: 268,000
.
.
. . .
Chronic lower
respiratory diseases: 66,000
28
Health&Science
Risk of second melanoma is higher than previously thought [ PAGE 33 ]
C
ardiovascular disease kills
nearly twice as many women
each year as does cancer, yet
annual mammograms and
Pap smears continue to be an
easier sell than lipid profiles or regular
blood pressure tests.
Despite years of warnings that women
face an even greater risk for cardiovascu-
lar disease than men, the word has been
slow to filter out. Women and their physi-
cians still don’t always acknowledge this
threat, nor do they take steps to slow its onset,
according to many experts. “It is really impor-
tant to keep educating patients and physicians
about this being such a devastating illness for
women,” said Norma Keller, MD, chief of cardiolo-
gy at Bellevue Hospital in New York City.
Figures from the Centers for Disease Control and
Prevention illuminate the problem. In 2003, 484,000
women died from cardiovascular disease compared with
427,000 men. Cancer, the next highest killer disease for
women, claimed 268,000 lives that same year.
The challenge for primary care physicians is to pick out
women most likely to benefit from treatment, said Lori Mosca,
MD, MPH, PhD, director of preventive cardiology at New
York-Presbyterian Hospital in New York City and chair of the
panel that drafted the American Heart Assn.’s Evidence-based
Guidelines for Cardiovascular Disease Prevention in Women.
“It is clear we are undertreating very high-risk women and
that there are many low-risk women who would be better
served by lifestyle changes than drug therapy.”
So how to determine which group is which? Go back to the
basics, she advises.
Evaluating traditional risk factors remains key for prima-
ry care physicians, Dr. Mosca said. “We have many physi-
cians who have not discussed with their patients their risk
factors for heart disease, including lifestyle and family histo-
ry.” Instead of preventive care, too many physicians are rely-
ing on technology that has not been proven to be associated
with beneficial outcomes, she added.
Jim King, MD, a family physician in rural Selmer, Tenn.,
keeps pushing this message to his female patients: “Watch
your cholesterol, blood pressure and weight, and don’t
smoke.” He notes that risk factors are the same for men and
women, although women’s risk starts to increase about
10 years later than men’s. His female patients also are
still more afraid of breast cancer. “They have to un-
derstand that heart disease is a more important
threat.”
The highest risk
African-American women are at the top of the risk
scale for heart disease, but they are the group least
likely to be diagnosed and treated effectively, said
Patricia Davidson, MD, a cardiologist at Washington
Hospital Center in Washington, D.C. “African-Ameri-
can along with Mexican-American and Native American
women have more risk factors lumped together.” Weight is a
problem. Sixty-eight percent of African-American women,
71% of Mexican-American women and 60% of Native Ameri-
can women are overweight, she noted. “With weight gain
comes insulin resistance, which leads to diabetes, which
raises your blood pressure.”
The lack of aggressive treatment to goal is another pitfall,
Getting to
the matter
the heartof
STORY BY SUSAN LANDERS
JUNE 5, 2006 AMEDNEWS.COM AMERICAN MEDICAL NEWS
SOURCE: CENTERS FOR DISEASE CONTROL AND PREVENTION AND
THE NATIONAL HEART, LUNG AND BLOOD INSTITUTE
PUBLIC HEALTH n CLINICAL ISSUES n PATIENTS
n Cardiovascular disease (CVD)
ranks first among all disease
categories in hospital dis-
charges for women.
n Of the approximately 5.5
million stroke survivors alive
today, 56% are women.
n Misperceptions still exist that
CVD is not a real problem for
women.
n CVD is a particularly
important problem among
minority women; the death
rate due to CVD is higher in
black women than in white
women.
n 38% of women compared with
25% of men will die within one
year after a heart attack.
SOURCE: AMERICAN HEART ASSN.
Cardiovascular death: 484,000
Alzheimer’s
disease: 45,000
Diabetes
mellitus: 39,000
LEADING CAUSES OF DEATH FOR WOMEN
in the United States, 2003
Cancer: 268,000
.
.
. . .
Chronic lower
respiratory diseases: 66,000
PHOTO ILLUSTRATION BY PETE MCARTHUR PHOTOGRAPHY](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-8-320.jpg)
![PAGE 9
1
Can we show
meaningful
comparisons?
MEDICATION
Methylphenidate,
amphetamine,
dextroamphetamine
Modafinil
Growth hormone
Testosterone
Nicotinic alpha-7
THERAPEUTIC INDICATION
Narcolepsy,
childhood ADHD
Narcolepsy, sleep apnea,
shift-work sleep disorder
Dwarfism, idiopathic
short stature, AIDS- and
cancer-related wasting
Hypogonadism,
andropause
Alzheimer’s,
schizophrenia
ENHANCEMENT USE
Intensify mental focus,
alertness
Combat jet lag, increase
wakefulness
Delay aging with increased
muscle, thicker skin, denser
bones, less total body fat
Delay aging with increased
muscle, denser bones,
better mood, higher libido,
enhanced cognition
Improve memory,
psychomotor skills
ETHICAL/SOCIAL CONCERNS
Social pressures could lead
to people using it to be
competitive
Could lead to compulsory
workplace doping to increase
effectiveness, safety
Could redefine aging as a
disease; stigmatize those
with short stature
Could redefine aging as a
disease; pose threat to
personal identity
Could present a greater
danger than enhancement
use of stimulants
SCOPE OF USE
Up to 25% of students at competitive
Northeastern universities reported
nontherapeutic use of stimulants
90% of prescriptions are for
off-label uses
About 30% of prescriptions are
for off-label uses
500% increase in total testos-
terone prescription sales have
been seen since 1993
At least 25% of people 85 and
older experience dementia; the
oldest of the country’s 75 million
baby boomers just turned 60
SOURCES: “DRUGS FOR ENHANCING COGNITION AND THEIR ETHICAL IMPLICATIONS: A HOT NEW CUP OF TEA,” EXPERT REVIEW OF NEUROTHERAPEUTICS, MARCH; “PROVISION
OR DISTRIBUTION OF GROWTH HORMONE FOR ‘ANTIAGING,’” JOURNAL OF THE AMERICAN MEDICAL ASSOCIATION, OCT. 26, 2005; “RISKS OF TESTOSTERONE-REPLACEMENT THERAPY
AND RECOMMENDATIONS FOR MONITORING,” NEW ENGLAND JOURNAL OF MEDICINE, JAN. 29, 2004; “SELECTIVE ALPHA7 NICOTINIC ACETYLCHOLINE RECEPTOR LIGANDS,” CURRENT
MEDICINAL CHEMISTRY, VOL. 13, NO. 13, 2006.
TREATMENTS TURNED ENHANCEMENTS GRAPHIC REPORTED BY KEVIN B. O’REILLY
The story discusses the quandaries emerging as some new treatments intended to heal the
sick are also being prescribed to enhance those who are healthy. The table and story work
together, with the text handling what experts are saying and the table highlighting the
types of drugs being discussed. The heavily-researched table adds a valuable dimension by
presenting factors at a level of detail that would have bogged down the story. The final two
columns (ethical/social concerns and scope of use) add meaningful content not available in
the story and describes the magnitude of the issue. The success of the graphic ultimately
rests in its ability to thoroughly present the essential details for a relevant list of drugs.
AMERICAN MEDICAL NEWS AMEDNEWS.COM AUGUST 28, 2006
11
Professional Issues
North Carolina considers limits on physician role in executions [ PAGE 13 ]
HEALTH CARE LITIGATION n MEDICAL EDUCATION n ETHICS n PROFESSIONAL REGULATION
TO HEAL, OR
TO ENHANCE?
L
ecturing a group of students last fall, Martha J.
Farah, PhD, commented that there was proba-
bly someone in the audience making use of
modafinil, approved to treat narcolepsy but
mostly prescribed off-label to long-haul truckers, jet-
lagged ocean hoppers and anyone else too busy to sleep.
“You were right about that!” said a graduate student
who approached Dr. Farah, director of the University of
Pennsylvania’s Center for Cognitive
Neuroscience, after the talk. Once a
week, said the student, who is also a
teaching assistant, he would find himself
falling behind on answering e-mail and
grading work. With modafinil, he could
stay up all night and still work through
the next day.
Dr. Farah’s observation was far from
a shot in the dark. Increasingly, students
at highly competitive universities such as Penn are us-
ing modafinil, or stimulants intended to treat attention-
deficit/hyperactivity disorder, to enhance their already
considerable abilities. Some students are asking doc-
tors for these so-called smart pills, though most obtain
them illegally from campus dealers.
College kids aren’t alone in looking to doctors to do
more than just cure their ills. Middle-aged men ask physi-
cians for testosterone boosters. Some adults even seek
growth hormones, one of the engines that allegedly
helped Barry Bonds overtake Babe Ruth on baseball’s all-
time home run list.
But should doctors say yes when patients ask for en-
hancement instead of healing?
It’s a question that medicine has grappled with on a
smaller scale for years. Cosmetic surgery posed similar
questions decades ago and continues to outpace med-
ically necessary reconstructive surgeries. Peter
Kramer’s 1993 book, Listening to Prozac,
alerted the nation to patients who sought
to feel “better than well.” And it didn’t
take long after Viagra’s 1998 approval be-
fore some normally functioning men be-
gan using the drug to enhance their sexu-
al experiences.
The question of whether to abide pa-
tient requests for enhancement treat-
ments will only continue to intensify as
new drugs hit the market. For example, Alzheimer’s
medication that is in the pipeline could potentially en-
hance healthy individuals’ memory.
In fact, the potential for genetic enhancement is so
great that the National Institutes of Health is funding
an investigation of the ethical implications of the re-
search. The AMA’s Council on Ethical and Judicial Af-
fairs also is studying human enhancement and may is-
sue ethical guidelines for physicians.
MAKING THE CALL
Doctors can be faced with
tough choices when
patients ask for something
to boost their abilities.
Franklin G. Miller, PhD, a
bioethicist at the National
Institutes of Health, and
Howard Brody, MD, PhD,
a family physician and
Michigan State University
bioethicist, offer two
principles to consider:
1. The more clearly an
intervention also
serves a legitimate medical
goal — such as preventing
disease, promoting health,
relieving pain and suffer-
ing, or avoiding premature
death — the more easily it
can be justified.
2. The greater the risks
involved, the more
difficult it is to justify an
enhancement intervention
in the absence of a clear
health rationale.
SOURCE: “ENHANCEMENT
TECHNOLOGIES AND PROFESSIONAL
INTEGRITY,” MAY-JUNE 2005
AMERICAN JOURNAL OF BIOETHICS
New treatments intended to
heal the sick also may help the
healthy flourish. Where should
doctors draw the line?
STORY BY
KEVIN B. O'REILLY
ILLUSTRATION BY
TED GRUDZINSKI
Continued on next page](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-9-320.jpg)
![PAGE 10
This story explores a study that
concluded doctors like the idea of
patient-centered care, but haven’t
adopted it. The story touches on
highlights from the study, while
the graphic allows readers to
do comparisons on a couple of
levels. First, the graphic shows
how three different groupings of
physicians ----- primary care,
specialists and all physicians -----
have adopted aspects of patient-
centered care. It also allows the
reader to quickly compare
numbers of how many have
adopted aspects vs. how many
say they plan to.
1
Can we show
meaningful
comparisons?
n A study reaching that conclusion comes
as some physician organizations are
trying to help practices redesign how they
provide care.
DAMON ADAMS
AMNEWS STAFF
Physicians are pretty good at providing same-day
appointments for patients who want them. And they
usually receive timely test results of patients they
referred to another doctor.
They don’t do as well at routinely using electron-
ic medical records or communicating with patients
via e-mail.
Those conclusions are based on what 1,837 physi-
cians, in practice at least three years, told re-
searchers. The nationwide survey led the authors of
a new study in the April 10 Archives of Internal Med-
icine to find that physicians favor such patient-cen-
tered care practices, but few practice all of them.
Physicians were asked about 11 patient-centered
practices, such as same-day appointments, e-mail
with patients, reminder notices for preventive or
follow-up care, electronic medical records and
patient survey feedback.
The study said that about one in four doctors us-
es electronic medical records and about half send
reminder notices to patients about preventive or fol-
low-up care.
Three in four primary care physicians had prob-
lems with the availability of patients records, test
results or other information at the time of a sched-
uled visit.
But researchers found that doctors favor many
elements of patient-centered care. The study said
87% of primary care physicians support improved
teamwork among health care professionals while
85% of all surveyed physicians favor easy access to
patients of medical records.
“They have the right attitude. They thought a
team approach to care was a good thing, and they’re
planning to look into electronic medical records,”
said lead study author Anne-Marie Audet, MD, vice
president for quality improvement at the Common-
wealth Fund, a private foundation in New York
City.
New models of care
The findings come at a time when some physician
organizations are making patient-centered care a
key component of efforts to redesign how physi-
AMERICAN MEDICAL NEWS AMEDNEWS.COM MAY 15, 2006
9
Professional IssuesHEALTH CARE LITIGATION n MEDICAL EDUCATION n ETHICS n PROFESSIONAL REGULATION
Some New York doctors join the Teamsters [ PAGE 14 ]
PUTTING IT INTO PRACTICE
A new study in the Archives of Internal Medicine found that a majority of physicians like
patient-centered care, but have adopted some aspects faster than others. Here is a look at some
patient-centered areas and the percentage of physicians who adopted the practices:
Doctors favor patient-centered
care but haven’t adopted it fully
“They thought a team approach to
care was a good thing, and they’re
planning to look into electronic
medical records.”
Anne-Marie Audet, MD, Commonwealth Fund
SOURCE: “ADOPTION OF PATIENT-CENTERED CARE PRACTICES BY PHYSICIANS,” ARCHIVES OF INTERNAL MEDICINE, APRIL 10 ISSUE.
Continued on page 13
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
PRACTICE ADOPTION PRACTICE ATTITUDE
A B C D E F
n Total physicians n Primary care physicians n Specialists
Local hospitals
could hold key to
boost residencies
n Increasing the physician work force
means training more residents, and a
medical school has found how to do so.
MYRLE CROASDALE
AMNEWS STAFF
After more than 20 years as a practicing gastroen-
terologist, Richard Greenwald, MD, is helping
turn his community hospital into a teaching
institution.
This year Dr. Greenwald, now vice president
of medical affairs at Boca Raton Community Hos-
pital, helped develop a module covering gastroen-
terology, the liver and nutrition for medical stu-
dents from the new University of Miami School of
Medicine program at Florida Atlantic University
in Boca Raton. The hospital’s partnership with
FAU and the University of Miami to teach med-
ical students is the first step in a long-range plan
to cultivate more physi-
cians for southeast Florida.
By 2010, some 100 to 125
medical residents are ex-
pected to be training there.
Boca Raton Community
Hospital may be the first
hospital in recent years to
take advantage of a little-
used opportunity to get
Medicare funding for new residencies. Because
the hospital has never sponsored a residency, it is
eligible for Medicare graduate medical education
dollars, money that has been capped for existing
programs since 1996.
Given concerns that a physician shortage may
develop by 2020, Boca Raton could become a mod-
el for those looking for ways to expand residen-
cies and physician numbers, work-force experts
say. Right now, opening residencies at hospitals
that haven’t previously had them is the only
route to get new government funding.
Richard Reynolds, MD, senior vice president
of medical advancement at Boca Raton Commu-
nity Hospital, wouldn’t be surprised if others fol-
lowed his hospital’s lead. “As we look ahead, with
the growth and aging of the population, we’re go-
ing to have a doctor shortage,” he said. “Current
schools are going to expand, and other [communi-
ty] hospitals will become teaching hospitals.”
Many consider such expansion good news. But
if more community hospitals do begin training
residents, some say the practice raises a broader
policy issue of how to best spend graduate med-
ical education dollars.
“Hospitals are feeling a need to increase resi-
dency size, and they aren’t getting the Medicare
funding to do it,” said Karen Fisher, senior asso-
ciate vice president of health care affairs at the
Assn. of American Medical Colleges. “If commu-
nity hospitals are interested in taking on GME,
that’s great. However, from a public policy per-
spective, wouldn’t it make more sense to expand
GME through quality existing programs as well
64 77 58 54 48 57 27 23 28 26 26 26 10 19 6 20 23 19
Continued on page 15
Med schools
expanding to
meet future
demand.
Page 17
A | Always or often provide a same-day appointment
to a patient who requests one
B | Send patients computerized or manual reminder
notices about regular preventive or follow-up care
C | Use electronic patient medical records routinely
or occasionally
D | Medical record(s), test results, or other relevant
clinical information never or rarely not available
at the time of patient’s scheduled visit
E | Plan to send reminder notices about regular
preventive or follow-up care within the next year
F | Plan to use electronic patient medical records
within the next year
PUTTING IT INTO PRACTICE
A new study in the Archives of Internal Medicine found that a majority of physicians like
patient-centered care, but have adopted some aspects faster than others. Here is a look at some
patient-centered areas and the percentage of physicians who adopted the practices:
SOURCE: “ADOPTION OF PATIENT-CENTERED CARE PRACTICES BY PHYSICIANS,” ARCHIVES OF INTERNAL MEDICINE, APRIL 10 ISSUE.
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
PRACTICE ADOPTION PRACTICE ATTITUDE
A B C D E F
n Total physicians n Primary care physicians n Specialists
64 77 58 54 48 57 27 23 28 26 26 26 10 19 6 20 23 19
A | Always or often provide a same-day appointment
to a patient who requests one
B | Send patients computerized or manual reminder
notices about regular preventive or follow-up care
C | Use electronic patient medical records routinely
or occasionally
D | Medical record(s), test results, or other relevant
clinical information never or rarely not available
at the time of patient’s scheduled visit
E | Plan to send reminder notices about regular
preventive or follow-up care within the next year
F | Plan to use electronic patient medical records
within the next year](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-10-320.jpg)
![PAGE 11
The success of this table is
largely due to the specificity
we provide with the data and
how it complements the main
story. Allowing the story
to focus primarily on the
potential versatility of this
type of employee, the graphic
addresses another key part of
the equation: Salary. The
graphic offers great depth by
showing average salaries
based on years of experience
as well as geographic region.
1
Can we show
meaningful
comparisons?
A
ccording the U.S. Bureau of Labor Statistics,
the fastest-growing health profession in the
country — the fastest-growing profession, pe-
riod — is medical assistant. Physicians such as
Catherine Tabb, MD, are one reason why.
Dr. Tabb, a solo family physician in Louisville,
Ohio, started practice in 1980 with one medical as-
sistant. She now has three full-time and three
part-time MAs. They’re used for all tasks — front,
as well as back office — not performed by her or
the practice’s single nurse practitioner.
Dr. Tabb likes the flexibility of staff who can
assume either front- or back-office duties to make
up for vacations or illness. But having people with
clinical knowledge at the front desk, making them
more useful to patients, is even better. “They can
answer basic questions about taking medications
without having to transfer the patient to me,” she
says. “They help patients decide if they need to
come in.”
Like most doctors who make extensive use of
MAs for clinical tasks, Dr. Tabb believes she’s in
no financial position to hire nurses. But more
than that, she says, they’re not necessary, particu-
larly when most of the clinical work can be
handled by MAs.
Charles Reed, MD, a pediatrician with 12-doc-
tor St. Christopher Pediatric Associates in
Philadelphia, says MAs bring versatility atypical
of other types of staff. “We can move them from of-
fice to office,” he says. “We can use them for clini-
cal tasks, and if we need to fill in, we can put them
in the front office, registering patients and an-
swering phones.”
The combination of versatility and compara-
tively low cost is driving the demand for MAs,
60% of whom work in physician offices. Accord-
ing to an American Assn. of Medical Assistants
survey of 4,057 MAs nationwide, 61.6% of an MA’s
time is spent on clinical duties, including obtain-
ing patient history and vital signs, assisting with
patient exams, scheduling patient appointments
and performing injections; 25.8% is spent on ad-
ministrative duties; 7.3% is taken up with admin-
istrative management; and 5.3% is spent on clini-
cal management. If they’re certified, MAs make
an average salary of $27,951. First-year MAs aver-
age $22,650, according to the AAMA.
Those in the field say doctors are just begin-
ning to tap the potential of MAs.
“Only a minority of physician groups know
how to utilize MAs and take full advantage of
what they can do,” says Don
Balasa, AAMA executive direc-
tor and chief counsel.
But hiring and integrating
MAs into your practice is not
necessarily an easy
task. The duties a me-
dial assistant can per-
form and the level of su-
pervision a physician
must provide can vary
depending on your state
and its regulations.
Generally, states
define what MAs
may or may not do
through scope-of-prac-
tice laws — if a task is
limited to a doctor, nurse
practitioner, physician as-
sistant or nurse, it’s off-
limits to an MA .
Finding a qualified MA
isn’t easy because of the
high demand. Another dif-
ficulty is that few have re-
ceived certification — estimates are at around
15% — through the AAMA or the American Med-
ical Technologists, giving physicians less evi-
dence an MA might be up to the job.
Hiring an MA
P
lenty of colleges and institutions offer two-
year programs for aspiring MAs. But doctors
vary on whether they require certification,
which is generally not required by law.
Dr. Tabb will hire only certified MAs.
Dr. Reed prefers but does not require a candi-
date to be certified. He typically hires only candi-
dates who have graduated from an accredited
post-secondary training program. In fact, most of
his hires are candidates who have completed in-
ternships in his office.
Nick Fabrizio is a consultant with MGMA Con-
sulting Group and serves as practice administra-
tor for a 12-doctor clinic that is part of the Dept. of
Family Medicine at State University of New York
Upstate Medical University, Syracuse. He says
the best way to find a good MA is to work with a
local educational organization that trains them.
His group works with Bryant & Stratton College,
a community college in Syracuse. By inviting stu-
dents to undertake internships at his group, “we
get to know the people intimately before we make
AMERICAN MEDICAL NEWS AMEDNEWS.COM APRIL 17, 2006
19
BusinessPRACTICE MANAGEMENT n PERSONAL FINANCE n TECHNOLOGY
Web site offers list of “average” costs of care [ PAGE 27 ]
Medical assistants
A key to practice efficiency
MAs can be the most versatile
members of your staff — if you
know how to use them.
Continued on next page
Story by Larry Stevens and Illustration by Terry Miura
MEDICAL ASSISTANT PAY
Here are overall and experience-based annual and hourly pay figures from the American Assn. of Medical
Assistants’ salary survey on medical assistant compensation. All figures below pertain to certified medical
assistants, a designation granted by the AAMA. The national average for noncertified MAs is $26,775, compared
with $27,951 for CMAs. Figures are as of 2004, the most recent survey.
New England (Conn., Maine, Mass.,N.H., R.I., Vt.) Annual $28,972 $25,056 $25,809 $29,219 $30,576
Hourly $14.49 $12.31 $13.08 $14.69 $15.22
Middle Atlantic (N.J., N.Y., Pa.) $30,451 $24,042 $28,710 $27,167 $32,341
$14.60 $12.96 $14.00 $13.34 $15.45
East North Central (Ill., Ind., Mich., Ohio, Wis.) $26,835 $22,128 $23,939 $25,070 $28,869
$13.27 $11.14 $11.98 $12.80 $14.15
West North Central (Iowa, Kan., Minn., Mo., $27,335 $23,150 $24,477 $26,900 $28,691
Neb., N.D., S.D.) $13.65 $12.04 $12.49 $13.53 $14.25
South Atlantic (Del., Fla., Ga., Md., N.C., S.C., $27,785 $22,922 $24,779 $26,972 $30,218
Va., W.Va., District of Columbia) $13.24 $11.53 $12.14 $13.05 $14.23
East South Central (Ala., Ky., Miss., Tenn.) $26,726 $22,000 $25,750 $25,974 $27,953
$12.69 $10.88 $11.78 $12.30 $13.29
West South Central (Ark., La., Ok., Texas) $29,115 * $24,600 $26,875 $31,152
$13.26 * $12.27 $12.54 $14.16
Mountain (Ariz., Colo., Idaho, Mont., Nev., $27,380 * $24,800 $25,426 $29,494
N.M., Utah, Wyo.) $13.40 * $12.58 $13.08 $13.98
Pacific (Alaska, Calif., Hawaii, Ore., Wash.) $29,995 $27,472 $27,082 $29,468 $31,534
$14.90 $13.76 $14.28 $14.94 $15.42
*INSUFFICIENT RESPONSE
NOTE: REGIONS ARE AS DEFINED BY THE U.S. DEPT. OF CENSUS.
SOURCE: AMERICAN ASSN. OF MEDICAL ASSISTANTS
REGION OVERALL 1–2 3–5 6–9 10 +
YEARS YEARS YEARS YEARS](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-11-320.jpg)
![PAGE 12
This was an ideal opportunity for a comparative
table. The story discusses an international patient
survey that showed the U.S. lagging behind five
other nations in nearly all areas surveyed. The
story described the nature of the survey and
provided numerous interesting findings, while
the graphic gave side-by-side rankings of the
six nations involved. At a glance, the reader can
compare rankings for the
subcategories that contribute
to the overall rank. Any story
that relies so heavily on
accessible comparisons like
these would suffer if it lacked
a graphic presentation of the
key findings.
1
Can we show
meaningful
comparisons?
n The country was rated
first only in
effectiveness of care.
ELAINE MONAGHAN
AMNEWS STAFF
Washington Adult patients in the
United States are less safe, not as
well informed by their doctors
and more unequally treated than
people in five other developed
nations that spend far less treat-
ing them, according to two stud-
ies released earlier this month
by the Commonwealth Fund.
America ranked last overall
when compared with Australia,
Canada, Germany, New Zealand
and the United Kingdom in one
study, “Mirror, Mirror, on the
Wall: An Update on the Quality
of American Health Care
Through the Patient’s Lens.”
This analysis compared U.S.
health leaders to the vain queen
in “Snow White.” Too often, they
excluded experiences of other coun-
tries, looking only “at our own reflec-
tion in the mirror,” the report states.
Based on 2004 and 2005 surveys, it
found that American patients were
most likely to say they encountered a
laboratory test mistake or delay in re-
ceiving abnormal results, did not get
questions answered by their physi-
cian, struggled to get needed care at
nights or on weekends, and failed to
fill or take prescriptions due to cost.
Janet Corrigan, PhD, president
and CEO of the National Quality Fo-
rum and the National Committee for
Quality Health Care, said the study
should not be read as an indictment of
physicians, but as further evidence of
the need to reform the country’s disor-
ganized health system. She noted
the study’s reliance on patient assess-
ments. “You might get different re-
sults if you asked physicians or
looked at medical records.”
The work, which followed an
Institute of Medicine framework
to evaluate health care system
quality, concluded that the Unit-
ed States ranked first in six out
of 51 indicators, and last or tied
for last in 27. Karen Davis, PhD,
the fund’s president, described
this outcome as “particularly
disturbing considering we lead
the world in health care spend-
ing.” The fund is a private health
foundation that supports re-
search into improving quality
and efficiency.
To arrive at its ratings, the
study used six categories:
l Patient safety addressed
wrong drugs or doses, mistakes
in care, and delayed or incorrect
test results.
l Effectiveness included use
of mammograms, flu shots, med-
ication reviews, diet and exercise
advice, hospital infections and
follow-up visits.
l Patient centeredness exam-
ined such issues as doctor communi-
cation, choice, time with the physi-
cian, pain management and access to
records.
l Timeliness addressed appoint-
ment wait times, emergency depart-
ment lines and access to care at irreg-
AMERICAN MEDICAL NEWS AMEDNEWS.COM APRIL 24, 2006
5
Florida passes bill limiting doctors’ share of liability [ PAGE 8 ]
MEDICARE / MEDICAID n LEGISLATION AND REGULATION n NATIONAL HEALTH POLICY
Government&Medicine
United States fares poorly in international patient survey
Continued on page 7
$40
$0
$60
$80
$100
Expenditures
(in billions)
’98 ’99 ’00 ’01 ’02 ’03 ’04 ’05
8.5% growth
in 2005
1.5% growth
in 1998
n The Centers for Medicare & Medicaid
Services also releases its projection of a
4.6% Medicare pay cut for doctors in 2007.
DAVID GLENDINNING
AMNEWS STAFF
Washington Although Medicare spending on physi-
cian services did not rise as much last year as it did
the year before, the increase was still large enough
to catch the attention of federal officials looking to
find more efficiency in the system.
The Centers for Medicare & Medicaid Services re-
cently estimated that spending on physician ser-
vices increased by 8.5% during 2005. In 2004, this
rate of growth was 11.4%.
But the nearly three percentage point drop was
not due to patients using fewer or less complex
Medicare services. Instead, the change is largely at-
tributable to decreased growth in beneficiary enroll-
ment, spending shifts stemming from the Medicare
drug benefit and lower reimbursement for physi-
cian-administered drugs and lab tests, CMS said.
All but one percentage point of the 8.5% increase
is due to physicians prescribing more services to
their Medicare patients and more intensive levels of
services. Physicians stepped up both the number
and complexity of basic services, such as follow-up
visits; minor procedures, such as physical therapy;
and screening tests, such as imaging scans.
The 16% growth in imaging service expenditures
alone, for example, was nearly twice as high as the
average rise in spending for all physician services.
Doctors’ greater reliance on CT scans and MRIs is
one of the biggest spending drivers in this area, the
agency said.
Such developments worry those who are charged
with making sure the program is paying for what it
views as the right patient care.
“Understanding the relatively rapid growth in
these services, and determining whether there are
ways to promote better health while slowing the
rapid increase in use of these services, is an increas-
ingly important issue,” wrote Herb Kuhn, director
of CMS’ Center for Medicare Management, in an
April 7 letter to the Medicare Payment Advisory
Commission.
PHYSICIAN SERVICES
Medicare expenditures under the physician
fee schedule in recent years have increased
by large enough percentages to catch the at-
tention of federal officials. With preliminary
numbers now in for 2005, here’s how spend-
ing has gone up over time:
SOURCE: CENTERS FOR MEDICARE & MEDICAID SERVICES
Medicare physician spending
growth worries U.S. officials
Continued on next page
HIGH SPENDING, LOW SCORE
The United States spends more per person on health care than any of the other
five countries studied, but it ranks last overall when scores for patient safety, ef-
fectiveness, patient-centeredness, timeliness, efficiency and equity are combined.
AUSTRALIA CANADA GERMANY NEW UNITED UNITED
ZEALAND KINGDOM STATES
OVERALL RANKING 4 5 1 2 3 6
Patient safety 4 5 2 3 1 6
Effectiveness 4 2 3 6 5 1
Patient-
centeredness 3 5 1 2 4 6
Timeliness 4 6 1 2 5 3
Efficiency 4 5 1 2 3 6
Equity 2 4 5 3 1 6
Per capita health
expenditures $2,903 $3,003 $2,996 $1,886 $2,231 $5,635
NOTE: BASED ON 2004 AND 2005 INTERNATIONAL HEALTH POLICY SURVEYS
SOURCE: COMMONWEALTH FUND, APRIL
HIGH SPENDING, LOW SCORE
The United States spends more per person on health care than any of the
other five countries studied, but it ranks last overall when scores for patient
safety, effectiveness, patient-centeredness, timeliness, efficiency and equity
are combined.
AUSTRALIA CANADA GERMANY NEW UNITED UNITED
ZEALAND KINGDOM STATES
OVERALL RANKING 4 5 1 2 3 6
Patient safety 4 5 2 3 1 6
Effectiveness 4 2 3 6 5 1
Patient-
centeredness 3 5 1 2 4 6
Timeliness 4 6 1 2 5 3
Efficiency 4 5 1 2 3 6
Equity 2 4 5 3 1 6
Per capita health
expenditures $2,903 $3,003 $2,996 $1,886 $2,231 $5,635
NOTE: BASED ON 2004 AND 2005 INTERNATIONAL HEALTH POLICY SURVEYS
SOURCE: COMMONWEALTH FUND, APRIL](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-12-320.jpg)
![PAGE 13
To balance a story about increases in Medicare
Part D prices, this graphic compares information
about specific drugs that doctors commonly
prescribe. The graphic gives doctors a sense of how
many health plans increased the cost of a particular
drug, what percent of plans decreased the price and
what the median percent change was. The chart
worked well because it offered tangible
information on drugs that readers commonly
prescribe. Had the information been integrated
into the story, it would have lost much of its utility.
1
Can we show
meaningful
comparisons?
n Pharmaceutical
manufacturers and
Medicare drug plans say the
studies misrepresent what
seniors are actually paying for
medications.
DAVID GLENDINNING
AMNEWS STAFF
Washington In the first three months
of the Medicare drug benefit, the
average wholesale price for roughly
200 of the brand-name drugs most of-
ten used by older Americans under-
went the single biggest jump in the
last six years, according to a recent
study by AARP.
The average price that drugmakers
charged wholesalers for medications
increased by 3.9% in the first quarter
of the year, four times the rate of gen-
eral inflation and the largest quarter-
ly increase since AARP began track-
ing the figures in 2000. For typical
people older than 50 taking four med-
ications per day, this means their av-
erage annual drug bills increased
roughly $240 over the 12 months lead-
ing up to the end of March, compared
with an increase of roughly $190 dur-
ing the previous year.
In a separate study, the consumer
group Families USA found that
Medicare drug plans are responding
to the wholesale price increases by
boosting what they charge for brand-
name medications. For the top 20
drugs prescribed to seniors, the vast
majority of Medicare Part D plans
quoted higher prices in mid-April
than they did in mid-November 2005,
when enrollment for the drug benefit
began.
The study showed that for 15 out of
the 20 medications, more than 80% of
the plans raised prices over that time
period, rather than lowering them or
keeping them the same. The median
percent change was 3.7%.
Both groups said that seniors are
being adversely affected because in-
surers are passing along the price in-
creases to beneficiaries.
“Shortly after the [Medicare drug
law] was enacted, AARP challenged
drug manufacturers to keep the rate
of price increase for drugs widely
used by older Americans to the rate of
general inflation,” the seniors’ group
said. “While the rate of increase did
slow down beginning in mid-2004, the
first quarter 2006 results represent a
disturbing reversal of that trend.”
Families USA Executive Director
Ron Pollack said the data in his
group’s report show that federal offi-
cials’ assertions about the power of
the market to drive prices down are
turning out to be wrong. Centers for
Medicare & Medicaid Services Ad-
ministrator Mark McClellan, MD,
PhD, Republican lawmakers and oth-
er drug benefit supporters have said
that private-sector competition would
do a much better job keeping costs in
check than government intervention.
“At the same time that the Bush ad-
ministration and congressional lead-
ers are touting the effectiveness of the
Medicare drug plans, those plans are
quietly raising the prices that they
charge,” Pollack said. “As a result, se-
niors will pay more and more — as
will America’s taxpayers.”
Both groups said that allowing the
federal government to negotiate with
drug companies over the prices they
charge, a task that is left to pharmacy
benefit managers in the private sec-
tor, would help alleviate cost spikes
such as the ones seen in recent
months. Such direct negotiation,
which would require congressional
approval, is supported by a range of
other groups, including the American
Medical Association.
More to the story
Drug manufacturers and Medicare
drug plans challenged both reports,
saying that the conclusions were
flawed and misleading.
Ken Johnson, senior vice president
for the Pharmaceutical Research and
Manufacturers of America, said that
more reliable official government da-
ta show recent drug prices tracking
the rate of increase in the costs of
medical products. Between January
and May of this year, that medical in-
flation figure was determined to be
JULY 10, 2006 AMEDNEWS.COM AMERICAN MEDICAL NEWS
10 Government & Medicine
WEBLINKS
http://www.familiesusa.org/
resources/publications/reports/
big-dollars-little-sense.html
“Big Dollars, Little Sense: Rising
Medicare Prescription Drug Prices,”
Families USA, June
http://www.aarp.org/research/
health/drugs/aresearch-
import-869-2004-06--IB69.html
“Trends in Manufacturer Prices of
Brand Name Prescription Drugs Used
by Older Americans — First Quarter
2006 Update,” AARP, June
Consumer groups report hike in Medicare Part D drug prices
Continued on page 12
PRESCRIPTION DRUG
PRICES ON THE RISE
In response to recently
increased medication prices
from pharmaceutical manu-
facturers, the vast majority of
Medicare drug plans between
November 2005 and April 2006
raised their listed prices for
the drugs physicians most
commonly prescribe to
seniors. Here is a sample of
those increases:
Drug Name % of plans that % of plans that Median percent
increased prices decreased prices price change
Zocor (40 mg) 100.0% 0.0% 5.7%
Fosamax (70 mg) 98.7% 1.3% 4.9%
Lipitor (10 mg) 97.3% 2.7% 6.5%
Xalatan (0.005 %) 96.8% 3.2% 4.9%
Toprol XL (50 mg) 96.2% 3.8% 3.0%
Actonel (35 mg) 96.1% 3.9% 4.9%
Celebrex (200 mg) 94.8% 5.2% 6.5%
Norvasc (5 mg) 94.6% 5.4% 3.2%
SOURCE: FAMILIES USA, “BIG DOLLARS, LITTLE SENSE: RISING MEDICARE PRESCRIPTION DRUG PRICES,”
JUNE](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-13-320.jpg)
![PAGE 14
Although not labeled as a “how to,”
this box gives readers tips on how a
doctor and patient can challenge an
insurer’s decision. Each bullet item
begins with a short declarative
sentence and is followed by a
description of what action to take. It’s
a good clip-and-save item, while the
story addresses in more depth how
physicians could use patients’ help
when appealing insurance decisions.
2
Can we offer
guidance
or tips?
How you and your patient
can successfully challenge
an insurer’s decision:
n Appeal every denial. Data
show appeals have a high
success rate.
n Record everything.
When you call an insurer
for preauthorization or veri-
fication of a benefit, make a
note of the conversation and
the names of people you
spoke with.
n Send all written correspondence via certified mail and keep
records. Time limits can be placed on insurers. Writing things
such as, “If you do not respond in five business days it will be as-
sumed there are no disputes with the content of this mailing”
can sometimes lead to quicker action.
n If you don’t get an acceptable answer, go up the chain of com-
mand. Copy the plan president with your dispute. For long-
standing disputes, send copies of your correspondence to the
state insurance commissioner or the state’s attorney’s office.
n Get the patient involved. A heartfelt letter explaining how the
patient’s life would improve with a certain procedure or treat-
ment can be compelling. If you anticipate difficulty, submit the
patient’s letter along with the initial claim.
n If another physician has more expertise that speaks to the
scope of the claim, include a second opinion.
n Establish a history with the patient and ensure it is well docu-
mented. Insurers place more weight on the opinions of a physi-
cian who has an established relationship with the policyholder.
n Get the employer or labor union involved. Experts say a com-
plaint from an employer who is paying for a large number of in-
surance plans gets attention.
Share the
heavy
lifting
AMERICAN MEDICAL NEWS AMEDNEWS.COM FEBRUARY 5, 2007
21
BusinessPRACTICE MANAGEMENT n PERSONAL FINANCE n TECHNOLOGY
Companies to fund new push for e-prescribing [ PAGE 26 ]
Insurance Disputes
Patients who deal directly
with insurers are often
more successful at resolving
disputes. But asking a
patient to intervene should
be a carefully considered
decision.
Harnessing
patient power
M
ark Granoff, MD, spent more than
an hour on the phone with an in-
surer trying to get approval for a
non-formulary medication. Three
separate phone calls and no head-
way later, he handed the prover-
bial baton to his patient.
Dr. Granoff, an internist and geriatrician
from Los Angeles, said he generally likes to
handle disputes himself. But in cases where he
clearly is getting nowhere, the former medical
director for Blue Cross of California knows
from experience that it’s the patient who holds
the power to get things done. Sometimes get-
ting the patient involved is key to getting a dis-
pute resolved.
Insurers “are not anxious to make the pa-
tient unhappy,” Dr. Granoff said. “They are
the ones paying.”
Getting a patient directly involved with in-
surance disputes can be tricky and can require
some coaching from the physician. But if done
at the right time and in an appropriate man-
ner, it can pay off.
Because patients have been paying more
out of pocket for their health care in recent
years, some doctors feel patients are more will-
ing to fight for benefits. And the time patients
spend advocating on their own behalf is time
physicians can devote back to patient care.
Kathryn Stewart, MD, MPH, a family physi-
cian and director of care management at Mt.
Sinai Medical Center in Chicago, said she used
to spend a lot of time on the phone advocating
for patients.
“But in this day and age, it’s just not practi-
cal for primary care physicians to do that any-
more,” Dr. Stewart said. “Doctors are in-
creasingly pressed to see more patients, and
many are having a difficult time staying
out of the red.”
While some have taken a proactive ap-
proach and gotten the patient involved
before a dispute arises, others have
found a patient’s voice can be the nudge
that results in a change of heart.
The people making the decisions “are
human, too,” said New York attorney
Richard Quadrino, who has represented
hundreds of doctors and patients in coverage
disputes.
When to get patients involved
T
he choice to get a patient involved should
be made judiciously, Quadrino said. “I
don’t know if the insurance company re-
ally wants to hear from the patient un-
less it’s a real medical necessity. And often the
doctor can speak to the medical issue.”
But Dr. Stewart said having communication
between the patient and the insurer can not on-
ly result in quicker resolutions to disputes in
certain situations, but can also be a good line
of defense if the patient is requesting a proce-
dure that the doctor knows will not be covered.
Because the patient is the client, “it’s really
up to the insurance company to explain to the
patient why or why not it is being covered,”
she said.
For example, she recently had a patient who
wanted to be transferred to a hospital outside
his HMO network. After a fruitless call to the
insurer, she told the patient he would have to
call the insurer directly if he really thought a
transfer should be granted.
Jerry Bridge, president of San Diego-based
Bridge Practice Management Group, encour-
ages physicians to anticipate potential prob-
lems and have new patients sign an appeals au-
thorization on their first visit. Having that
Continued on next page
Story by Pamela Lewis Dolan
Illustration by Jem Sullivan](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-14-320.jpg)
![PAGE 15
According to an IOM panel report, 1.5 million
people are harmed annually by medication
errors. This story explains the panel’s findings
and more importantly, provides something the
reader can act on: Guidance on how physicians
can reduce some of those errors. Presented under
a direct headline, “What you can do to reduce
errors,” this box delivers 13 tips from the IOM
report in simple, useful language. Many reports
and studies outline problems, but no answers.
This is a strong example of providing both.
A CLOSER LOOK AT THE MONEY
Commercial entities — pharmaceuti-
cal companies and medical device
manufacturers — poured a record
amount of money into continuing
medical education and related
education activities in 2005. Propor-
tionally, however, their dollars
accounted for a smaller piece of the
overall CME
n A panel’s report calls on all physicians
to prescribe electronically by 2010, but
experts say that’s a reach.
KEVIN B. O’REILLY
AMNEWS STAFF
At least 1.5 million people are injured annually by
preventable medication errors that occur at every
stage of the process, from prescribing to dispensing
to patient administration, according to a July Insti-
tute of Medicine report.
The new report says physicians, nurses, pharma-
cists, patients and drugmakers must work together
to combat the many factors that contribute to the
persistence of these errors, which the IOM earlier
reported kill an estimated 7,000 people a year.
“The 1999 report [“To Err is Human”] raised
awareness about errors in general,” said J. Lyle
Bootman, PhD, ScD, co-chair of the IOM Committee
on Identifying and Preventing Medication Errors
and dean of the University of Arizona College of
Pharmacy. “The current report makes clear that we
still have a long way to go.”
Albert W. Wu, MD, MPH, a panel member and
professor of health policy and management and in-
ternal medicine at Johns Hopkins University in
Baltimore, said the report’s findings make clear
that medication errors are the most far-reaching of
medical errors.
“I’m a patient-safety researcher, and even as we
went through the process I was surprised by just
how common and how serious a problem this is,”
Dr. Wu said. “We all need to wake up and take a part
in fixing it.”
Most important for physicians, the panel called
on all prescribers to have a plan to implement an
electronic prescribing system by 2008 and to have
such systems in place by 2010.
Wilson D. Pace, MD, a panel member and Green-
Edelman Chair for Practice-based Research at the
University of Colorado, said even the most talented
physicians need electronic systems to help them
prescribe safely.
“With 15,000 medications available, it’s virtually
impossible to track all of those anymore just using
your memory,” Dr. Pace said. “Electronic prescrib-
n But at the local level, some
CME providers say they
have found that there’s less in
the pot for them.
MYRLE CROASDALE
AMNEWS STAFF
Spending on continuing medical edu-
cation over a one-year period was up
nearly 10% in 2005, to $2.25 billion, but
a smaller percentage of that money
came from pharmaceutical compa-
nies and other commercial interests
than in years past, according to the re-
cently released 2005 annual report of
the Accreditation Council for Contin-
uing Medical Education.
Commercial interests — drug com-
panies and medical device manufac-
turers — increased their giving to
CME providers to $1.35 billion in 2005
for such items as education grants
and exhibit space.
But because of increased money
from registration fees and noncom-
mercial groups, the share of spending
by pharmaceutical and device manu-
facturers covering CME costs as well
as CME-related advertising and ex-
hibit fees fell from 62% in 2004 to 60%
in 2005.
Part of this decrease is also attrib-
uted to ACCME changing the defini-
tion of commercial support to exclude
money or services from nonprofit or
government organizations and non-
health care-related companies.
Increased total spending in 2005 al-
so translated into an increased num-
ber of total CME activities, with the
national specialty societies and large
CME providers still capturing a sig-
nificant portion of pharmaceutical
dollars.
Despite the net increase on paper,
locally produced CME is facing a re-
duction in commercial educational
grants as state medical societies and
small- and mid-sized hospitals capture
a smaller share of commercial CME
support, some experts say.
With pharmaceutical and device
manufacturers the largest contribu-
tors to educational activities for prac-
ticing physicians, say the experts, this
could signal a reduction in the
amount of CME available for physi-
cians at the local level.
Murray Kopelow, MD, ACCME
chief executive, said he’s heard from
CME providers that commercial CME
funding is falling, particularly on the
local level, but said the ACCME does
not capture data at the local level.
AMERICAN MEDICAL NEWS AMEDNEWS.COM AUGUST 21, 2006
9
Professional IssuesHEALTH CARE LITIGATION n MEDICAL EDUCATION n ETHICS n PROFESSIONAL REGULATION
Calif. high court shields peer reviewers [ PAGE 13 ]
MEDICATION ERRORS ADD UP
The toll of preventable medication errors
is uncertain, but in a July report, an
Institute of Medicine panel estimates that
at least 1.5 million people are harmed an-
nually by preventable medication errors.
Here’s a breakdown of these estimates:
400,000preventable
drug-related
injuries occur each year in hospitals.
It costs an extra $3.5 billion to treat those
injuries.
800,000preventable
drug-related
injuries occur in long-term care settings.
530,000preventable
drug-related
injuries occur among Medicare recipients
in outpatient clinics. In 2000, it cost $887
million to treat those injuries.
25%of all medication errors are
due to similar drug names.
33%of drug errors, including
30% of deaths, are due to poor
labeling and packaging.
E-prescribing urged as one
error-prevention strategy
More dollars flow into continuing medical education
Continued on next page
Medication mix-ups prevalent
Continued on page 12
$0.0
$0.5
$1.0
$1.5
$2.0
$2.5
2003 2004 2005
BILLIONS OF DOLLARS SPENT
$2.25
$2.05
$1.77
60%
62%
65%
35%
38%
40%
CME FUNDING
Including pharmaceutical and
medical device manufacturer
spending, physician registration fees
and other sources of income.
WHERE CME DOLLARS CAME FROM
n Commercial entities
n Registration fees and other
noncommercial CME income
HOW COMMERCIAL SPENDING BREAKS DOWN
Education, Advertising, Physician fees,
grants, support exhibit income other income
2003 55% 10% 35%
2004 52% 10% 38%
2005 50% 10% 40%
SOURCE: ACCME 2005 ANNUAL REPORT
WHAT YOU CAN DO TO REDUCE ERRORS
A July Institute of Medicine report says office-based physicians should take these steps
to minimize medication errors:
n Put an electronic prescribing plan in place by 2008; implement e-prescribing by 2010.
n Reconcile medications at transition points — admission, discharge and transfer.
n Create a routine to reconcile medication changes with the pharmacy record.
n Keep an accurate medication list for each patient, including over-the-counter and
complementary and alternative medications. Ask patients to bring their medications in
periodically to keep the list up to date.
n Do the following when prescribing new medication: Ask about allergies, inform the
patient of indications for all medications, explain common or significant side effects,
consult electronic or other reference sources for questions, avoid abbreviations and in-
clude patient age and weight when applicable.
n Ask regularly whether patients are taking their medications, including as-needed
drugs. If they aren’t taking the medication, it may signal that a patient had an adverse
reaction to the drug.
n Monitor the patient for response to medication therapy and ask regularly about side
effects or adverse drug events.
n Standardize communication about prescriptions within the practice; standardize and
improve handoffs to the primary pharmacist.
n Ask the primary pharmacy about the patient’s refill history.
n Work as a team with the primary pharmacist and nurses.
n Minimize the use of free samples; when dispensing free samples, apply standards
similar to those a pharmacy would use.
n Exercise particular caution in high-risk situations, such as times when a physician is
stressed, sleep-deprived, angry or is supervising inexperienced personnel.
n Report errors and adverse drug events to the Medication Errors Reporting Program,
jointly run by U.S. Pharmacopeia and the Institute for Safe Medication Practices as well
as the appropriate patient-safety organization or authority, depending on the state.
2
Can we offer
guidance
or tips?](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-15-320.jpg)
![PAGE 16
STANFORD’S RULES
Medical staff, faculty, students and trainees at the Stanford University
School of Medicine, Stanford Hospital and Clinics and the Lucile
Packard Children’s Hospital must follow these standards:
n No personal gifts of any size from industry, under any circumstances.
n No compensation for listening to a sales talk.
n No compensation — including defraying costs — for attending
a continuing medical education event or other activity, unless an
individual is presenting at the event.
n No sales representatives in patient-care areas, unless it’s to train staff
for research or on how to operate clinical equipment. All visits must be
by appointment.
n No sales representative visits with physicians without an appoint-
ment. These appointments may be made at the physician’s discretion.
n No industry support directly to students and trainees. The support
must be provided through the school and must be free of any actual or
perceived conflict of interest and specifically for educational purposes.
SOURCE: STANFORD UNIVERSITY SCHOOL OF MEDICINE
2
Can we offer
guidance
or tips?
For this page 1 story, Stanford is the first school
highlighted in an exploration of academic medical
centers taking firmer stances against pharmaceutical
marketing efforts on campus. It is not until well into
the jump that other institutions are discussed at length,
so it makes sense that Stanford’s rules get prominence.
The guidelines staff and students must follow are already
written clearly and make a compelling graphic about
real-world expectations. The story gets into the policies
of other schools and changes that have come about in
response and also offers a graphic on the JAMA article
challenging academic
medical centers to take the
lead on conflict-of-interest
reforms. Providing
Stanford’s clearly stated
guidelines helps the story
become more tangible.
n Stanford, Yale and the
University of Pennsylvania
have adopted policies to create
a brighter line between medicine
and marketing.
MYRLE CROASDALE
AMNEWS STAFF
On Oct. 1, Stanford University School
of Medicine in California closed its
last avenue for pharmaceutical mar-
keting on campus, shutting down
drug company freebies no matter
what their size.
The ban includes everything from
free lunches to pens touting the latest
medication to hit the market. Also,
pharmaceutical sales representatives
must make appointments if they want
to talk with physicians. The stricter
rules come after the school prohibited
drug samples several years ago, ex-
cept at medical students’ free clinics.
Stanford is one of a handful of acad-
emic medical centers expanding con-
flict-of-interest rules beyond research
to include smaller gifts aimed at influ-
encing physicians’ clinical practices,
namely prescribing.
Although there is no hard number
on how much is spent, Stanford esti-
mates that drug companies lay out
about $250,000 annually on meals
there. Nationwide, the pharmaceuti-
cal industry estimates that it spends
$21 billion a year on marketing,
though some contend that this figure
is too low.
“There’s a growing awareness that
pharmaceutical promotions subtly,
and not so subtly, impact physicians’
decisions,” said internist Clarence
Braddock, MD, MPH, an associate
professor at Stanford and a member of
the Stanford Center for Biomedical
Ethics. “Even if [you believe] there’s
www.amednews.com
AMERICAN MEDICAL NEWS
515 NORTH STATE
CHICAGO, IL 60610
★ ★ ★
CLASSIFIED ADVERTISING – PAGES 37-38
October 9, 2006
VOLUME 49 n NUMBER 38American Medical
Souped-up EMR
Physicians who want to
integrate a patient’s genetic
code into treatment using
bioinformatics need the
technology and ability to
analyze the data.
In Business, page 21
Specialty hospital fight
goes to state’s high court
Government & Medicine, page 7
Online prescribing
spurs criminal charges
Professional Issues, page 16
Hospital competition
breeds quality
Opinion, page 30
Doctors wary about
flu vaccine deliveries
Health & Science, page 32
Promise and
challenges
In the last of a three-part
series, doctors try to look
beyond today’s crisis and see
what lies ahead in fixing the
Medicare pay system.
In Government & Medicine, page 5
Cancer, families
and physicians
The book A Lion in the House
features insights from parents,
doctors and others who cared
for five children at a
Cincinnati hospital.
In Professional Issues, page 12
Restricting drug reps
Some medical schools say no to free lunch
Physician service growth rate slows,
easing Medicare premium increase
STANFORD’S RULES
Medical staff, faculty, students and trainees at the Stanford University
School of Medicine, Stanford Hospital and Clinics and the Lucile
Packard Children’s Hospital must follow these standards:
n No personal gifts of any size from industry, under any circumstances.
n No compensation for listening to a sales talk.
n No compensation — including defraying costs — for attending
a continuing medical education event or other activity, unless an
individual is presenting at the event.
n No sales representatives in patient-care areas, unless it’s to train staff
for research or on how to operate clinical equipment. All visits must be
by appointment.
n No sales representative visits with physicians without an appoint-
ment. These appointments may be made at the physician’s discretion.
n No industry support directly to students and trainees. The support
must be provided through the school and must be free of any actual or
perceived conflict of interest and specifically for educational purposes.
SOURCE: STANFORD UNIVERSITY SCHOOL OF MEDICINE
Continued on next page
n Meanwhile, beneficiaries
with higher incomes will pay
bigger premiums next year as
the result of a 2003 law.
DAVID GLENDINNING
AMNEWS STAFF
Washington Medicare beneficiaries next
year will not see their premiums rise
as much as originally thought now
that federal officials have downgraded
their projections of how much doctor
care is costing the program.
The standard 2007 monthly premi-
um for Medicare Part B, which covers
outpatient physician care, will in-
crease by $5 to $93.50. The Centers for
Medicare & Medicaid Services esti-
mated in July that the premium
would jump by nearly $10 to $98.40.
The new figure will be the smallest in-
crease in six years.
Beneficiaries will pay less because
federal officials have revised the rate
at which spending on physician care
is increasing, said CMS Administra-
tor Mark McClellan, MD, PhD. In par-
ticular, the growth rate for physician
services in 2005 slowed compared
with recent years, altering projec-
tions for the future.
CMS originally thought that the
amount of services that doctors were
billing was spiking, but now officials
have realized that doctors simply were
filing claims more efficiently and re-
ceiving payments more quickly. The
effect of the higher efficiency made it
look to actuaries as if doctors were
boosting the total level of care they
were prescribing to their patients.
The amount that seniors are ex-
pected to pay to receive coverage un-
der the program is dependent in part
on the amount and complexity of ser-
vices that doctors provide. Because
Part B premiums are calculated to
cover 25% of the program’s costs, any
increases in physician services result
Continued on page 4](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-16-320.jpg)

![PAGE 18
The Blair Law Firm LLC of
Scottsdale, Ariz., which repre-
sents medical directors and
physician entrepreneurs, lists
online what doctors need to con-
sider before casting their lot with a medical fran-
chise (http://www.retailmedicine
law.com/8_things/):
1.Asset protection. The firm’s advice: Never
enter into a consulting or franchise agreement
in your own name, or in the name of your practice.
Not unless you want your own personal or practice
assets in play if legal issues come up with the fran-
chise.
2.Health and medical laws and regulations.
You need to know the state regulations gov-
erning the practice of medicine — and assume they
will get stricter. Also, you need to know your
state’s corporate practice of medicine doctrine. At
the least, that doctrine might require you to set up
multiple legal entities for your franchise, which
technically is a lay corporation practicing medi-
cine. You also must be aware of fee-splitting regula-
tions, which prevent a lay corporation from shar-
ing in the income of a physician’s practice, as well
as HIPAA privacy and security regulations. You al-
so need to know what the facility licensing laws are
in your state.
3.Medical directors as adversaries and
partners. As the firm puts it, whether you
are an owner, franchisee or an area developer, care
must be taken in the recruitment, employment,
compensation and termination of medical direc-
tors. There are no standardized agreements to em-
ploy a medical director, so they will vary based on
the state’s legal requirements
and the franchise’s own opera-
tional requirements.
4.Advertising and ethics. A
potential franchiser might
use enhanced and idealized images, models, “be-
fore and after” photos and other advertising that is
contrary to traditional medical ethics. You should
have independent advertising and marketing pro-
tocols in place to ensure that any advertising does
not conflict with those ethics.
5.Insurance coverage. You’ll need it. Lots of
it. And lots of varieties of it. For example,
Blair points out that a medical spa franchise will
need medical professional liability insurance, med-
ical spa liability insurance, general business liabil-
ity insurance, employee benefits liability insur-
ance, group health insurance, directors and
officers insurance, workers’ compensation insur-
ance and employment practices insurance.
6.Franchise business models. Remember
how hot Krispy Kreme Donuts franchises
were? Well, now some in the U.S. and Canada have
filed for bankruptcy protection because of the com-
pany’s woes, which include a Securities and Ex-
change Commission investigation into the compa-
ny’s accounting. Blair says physicians need to
remember most franchises are “dynamic” — mean-
ing that turns in the market or failures of manage-
ment can turn things sour quickly, and at any time.
Mainly this is because, as Blair says, companies
choosing to franchise usually do so because they
are thinly capitalized and thus cannot raise money
for expansion through other methods. So a fran-
2
Can we offer
guidance
or tips?
AMERICAN MEDICAL NEWS AMEDNEWS.COM SEPTEMBER 25, 2006
19
BusinessPRACTICE MANAGEMENT n PERSONAL FINANCE n TECHNOLOGY
HCA, United go head-to-head over pay rates [ PAGE 25 ]
The Blair Law Firm LLC of
Scottsdale, Ariz., which repre-
sents medical directors and
physician entrepreneurs, lists
online what doctors need to
consider before casting their lot
with a medical franchise
(http://www.retailmedicinelaw.
com/8_things/):
1.Asset protection. The
firm’s advice: Never enter in-
to a consulting or franchise
agreement in your own name, or
in the name of your practice. Not
unless you want your own per-
sonal or practice assets in play if
legal issues come up with the
franchise.
2.Health and medical laws
and regulations. You need
to know the state regulations gov-
erning the practice of medicine —
and assume they will get stricter.
Also, you need to know your
state’s corporate practice of medi-
cine doctrine. At the least, that
doctrine might require you to set
up multiple legal entities for your
franchise, which technically is
a lay corporation practic-
ing medicine. You also
must be aware of fee-
splitting regulations,
which prevent a lay
corporation from
sharing in the income
of a physician’s prac-
tice, as well as HIPAA
privacy and security regula-
tions. You also need to know
what the facility licensing laws
are in your state.
3.Medical directors as ad-
versaries and partners.
As the firm puts it, whether you
are an owner, franchisee or an
area developer, care must be
taken in the recruitment, em-
ployment, compensation and ter-
mination of medical directors.
There are no standardized agree-
ments to employ a medical direc-
tor, so they will vary based on
the state’s legal requirements
and the franchise’s own opera-
tional requirements.
4.Advertising and ethics. A
potential franchiser might
use enhanced and idealized im-
ages, models, “before and after”
photos and other advertising that
Risky Business
fter nine years in practice, Brent
Greenberg, MD, was fed up with the
hassles that come with the business of
medicine. So he decided to look for
something that would complement his
work and still generate revenue.
What he found was a skin-care clinic franchise look-
ing for physicians to own outlets. In August, Dr.
Greenberg and another physician paid a $75,000 fran-
chise fee to open Dermacare of Rancho Bernardo, a
laser aesthetic skin care franchise in San Diego.
Dr. Greenberg, a family physician in Escondido,
Calif., said the franchise was consistent with his inter-
est in skin care — and his interest in gaining control of
his practice’s future by finding something to buttress
the reimbursement cuts his practice is seeing.
“For me going into this area, it’s part of the despera-
tion factor. I’m tired of working 14-hour days,” he said.
It appears that more and more franchises are reach-
ing out to physicians who think the same way. These
franchises offer the chance to launch a medical spa,
skin-care center, weight-loss facility, smoking cessa-
tion center or other services perceived to be in high de-
mand by cash-paying patients.
In return, physicians pay a franchise fee and a por-
tion of all revenue. Also, the physician agrees to oper-
ate under the franchiser’s rules. There isn’t the free-
dom of an independent business, but franchisers say
there aren’t as many of the hassles — including build-
ing up a brand name.
There are no exact numbers on franchises with
physician owners, but a quick Web search turns up nu-
merous results for chains pitching to physicians.
Hannelore Leavy, founder and executive director of
the Union City, N.J.-based International Medical Spa
Assn., said although the industry didn’t really take off
until four years ago, there are now nearly 1,500 med-
ical spas operating in the United States, about a quar-
ter of which are franchises.
Dr. Greenberg’s franchiser, Phoenix-based Derma-
care Laser & Skin Care Clinics, says it has about 150
franchises nationwide, all owned by doctors, and it is
growing quickly.
“Investing in one of our franchises provides a cash-
based opportunity for physicians to generate revenue
and still practice medicine without the insurance reim-
bursement headaches associated with a traditional
In light of declining reimbursements and greater workloads, the idea of an outside
company setting you up with a brand-name medical side business might sound good.
But there are many things to think about before taking the plunge.
STORY BY KATHERINE VOGT l ILLUSTRATION BY GRADY MCFERRIN
Continued on next page
THINGS TO KNOW
BEFORE BUYING
A FRANCHISE
Continued on next page
THINGS TO KNOW
BEFORE BUYING
A FRANCHISE
Continued on page 19
This graphic delivers exactly
what its headline touts. The
story gets into the physician
experience and ethics
regarding franchises, while
this box, accompanied by a
second one of FAQs, provides
the detailed guidance. The
graphic, a list modified from
information from legal experts
who specialize in this area,
provides the needed authority.
The graphic and story have
minimal content overlap, so
each piece is essential to the
overall storytelling.](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-18-320.jpg)
![PAGE 19
2
Can we offer
guidance
or tips?
This feature tells personal stories of
doctors worried about a new Medicaid
citizenship test. The Documentation
Details box gives physicians quick-hit
information about the law. It uses a
device that clearly outlines the questions
a doctor might ask and gives the answers
— for example “who must show proof”
and “who is exempt.” It would be an easy
item for a doctor to clip and save.
AMERICAN MEDICAL NEWS AMEDNEWS.COM AUGUST 7, 2006
5
Doctors fear that Medicare hospital payment changes could hurt care [ PAGE 9 ]
MEDICARE / MEDICAID n LEGISLATION AND REGULATION n NATIONAL HEALTH POLICY
Government&Medicine
T
he federal government last month
eased the new requirement that Medic-
aid recipients prove their U.S. citizen-
ship. But the changes won’t help
everyone, say doctors who treat these patients.
Take David Bell, for example.
About 65 years old, Bell was born into 1940s
Alabama. The son of sharecroppers, he says he
was one of about 16 children in his family. His
mother died when he was small. Like his sib-
lings, with whom he has no contact, he was not
born in a hospital. He has no birth certificate.
“We grew everything — cotton, corn, peanuts,
cucumbers,” the soft-spoken man said in an in-
terview in the waiting room of the medical clinic
at Bread for the City, a community health center
in Washington, D.C., that serves many low-in-
come Medicaid recipients. “By being so many of
us, we went hungry most of our lives.”
The law, which took effect July 1, mandates
that individuals seeking care through Medicaid
show proof of U.S. citizenship, such as a birth
certificate, passport or other acceptable form of
identification. The measure, signed by Presi-
dent Bush in February as part of the Deficit Re-
duction Act, is supposed to prevent illegal immi-
grants from abusing the system.
But many doctors argued that the real vic-
tims would be millions of impoverished Ameri-
cans, particularly elderly black patients, and
that the law was unnecessary.
“People are not trying to get around the sys-
tem,” said Randi Abramson, MD, the medical di-
rector at Bread for the City, which provides a
variety of services to the needy, including food.
“In reality, most people tell the truth.” Her as-
sessment of the law: “It’s built on fear and based
on nothing.”
The federal government last month changed
the citizenship requirement to exempt people al-
ready enrolled in Medicare or receiving Supple-
mental Security Income. The Centers for
Medicare & Medicaid Services estimated that
this exemption would cover about 8 million of
the roughly 55 million people in Medicaid.
Bell is just the type of person the move aimed
to help. But he is not enrolled in Medicare and
doesn’t receive SSI, so he’s still out of luck.
“I’m a survivor, with these tools,” Bell said,
slowly turning the palms of his rough hands up-
ward. “I still have the spirit and the
blessing, and I do what I have to do to
survive.”
Bread for the City helps him with
his diabetes medication. But he has to
use far cheaper, older drugs that are
managing the disease now but usually
prove less effective.
Bell is a long way from producing
the documents that would let him ac-
cess Medicaid and other federal pro-
grams despite years of struggle to es-
tablish his identity with the help of
lawyers at a local church and at Bread
for the City. The clinic has gotten as
far as obtaining school records from Alabama,
but they don’t match Bell’s belief that he was
born on Oct. 26, 1941. Without a witness to con-
firm his birth date, one of the alternative routes
to proving his identity under the new law, he
has nowhere to turn.
“Are they going to believe you or the school
record? That’s going to be the lawyer’s next
problem,” Dr. Abramson said. “The school
record is clearly wrong. It includes two kids
born four months apart.”
She added that the law should have allowed
for simple interviews to establish the patient’s
citizenship.
Dr. Abramson said the Supplemental Securi-
ty Income and Medicare exemption would be a
big help for many of the patients who were wor-
ried about the citizenship requirement. But, she
added, the development is of little comfort to
Bell or a number of her other patients, such as
low-income pregnant women, who don’t fit that
category. She said her center will continue to
see people without documentation, but their ac-
cess to specialists or prenatal care will be hurt.
Savings at what cost?
The Congressional Budget Office has estimated
that the new law will save the federal govern-
ment $220 million over five years and $735 mil-
lion over a decade, with about 35,000 people,
mostly undocumented immigrants, losing cov-
erage by 2015. But the Center on Budget and Pol-
icy Priorities, a nonprofit group that analyzes
fiscal policy issues, estimated before CMS an-
nounced the exemption that between 3 million
and 5 million people could lose coverage be-
cause they lack documentation.
Judith Solomon, a senior fellow at the center,
said at the time that between 1.4 million and 2.7
million children would be affected by the law.
Citizenship Test?
WILL MedicaidFAIL ITS
Doctors worry that a law aimed at preventing illegal immigrants
from getting program benefits will instead hurt access for lawful residents.
Story by Elaine Monaghan, Photos by Mark Finkenstaedt
“People are not
trying to get around
the system. In reality,
most people tell
the truth.”
RANDI ABRAMSON, MD
Medical director, Bread for the City
Continued on next page
s
DOCUMENTATION DETAILS
New federal rules require that Medicaid
patients prove their status as a U.S.
citizen or a legal immigrant. Here is
a snapshot of some of the recently
announced guidelines of the Centers
for Medicare & Medicaid Services.
Who must show proof: Currently enrolled
Medicaid patients at the time they renew
their benefits; first-time qualified patients
at the time they apply.
Who is exempt: Seniors and disabled
patients who receive Medicare or
Supplemental Security Income.
Acceptable forms of citizenship proof:
U.S. passport, certificate of naturalization,
certificate of U.S. citizenship, U.S. birth
certificate or data matches with state vital
statistics agencies, if available.
Additional forms of citizenship proof:
In rare circumstances, a written affidavit
by two individuals who have personal
knowledge of the patient’s citizenship, one
of whom cannot be related to the Medicaid
patient.
Acceptable forms of identification that
must accompany citizenship proof:
Current state driver’s license or other
picture ID card issued by a federal, state
or local government agency, or data
matches with other government agencies.
SOURCE: CENTERS FOR MEDICARE & MEDICAID SERVICES
chisee needs to study the company and its
management closely before making an in-
vestment, including looking at management
turnover (the more turnover, the more you
should be cautious) and understanding the
company’s long-term business model.
7.Systemic franchise litigation. This
means that a legal action against one
franchisee could close down an entire fran-
chise system. Blair recommends that every
retail medicine franchise agreement (and re-
lated commercial lease agreements) should
contain bailout provisions in the event of sys-
temic third-party litigation.
8.Regional franchises and area devel-
opers. It sounds a little bit Amway —
not only do you get a franchise, but you also
get the rewards of finding other physicians in
your area to open franchises as well. Blair
notes that this can make you more money,
but it also carries a lot more risk. At the least,
if you fail to develop an area sufficiently, you
could face legal action from the franchiser
and the other franchisees — even if the fran-
chiser goes out of business. u
— Katherine Vogt](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-19-320.jpg)
![PAGE 20
2
Can we offer
guidance
or tips?
This feature discusses the high
probability that a physician will
face an employee struggling
with alcohol or substance abuse.
The box accompanying it gives
physicians signs that may
indicate a substance abuse
problem. The story weaves in
some of the content from the
graphic, but the list’s quick and
to-the-point nature provides
doctors with a handy checklist.
I
F ALL THE STATISTICS ARE TO
be believed, there’s a chance
your practice at some point
could have an employee, per-
haps even a physician, struggling
with drug or alcohol abuse.
It can be an issue for your prac-
tice beyond merely the perfor-
mance and health of one employee.
An employee’s substance abuse
problem can have a negative im-
pact in terms of decreased produc-
tivity, absenteeism, turnover and
medical costs. It also has the added
impact in a physician’s office of po-
tentially harming patients.
If an employee has a problem, or
if you even suspect an employee
has a problem, your instinct might
be to act on it quickly. But you face
a thicket of ethical and legal ques-
tions that could leave you with no
simple solution in dealing with it.
On one hand, you want to do
everything you can to protect pa-
tients from any harm the employee
could cause. On the other, employee
privacy issues, Americans with Dis-
abilities Act regulations and even
the high cost of training a new
worker come into play in how to
treat an employee who might have a
substance abuse problem.
“You’re not going to throw
someone away for asthma or dia-
betes,” says Harold Urschel, MD,
an addiction psychiatrist in Dallas.
Substance abuse, he says, must be
treated the same way.
Experts say there are two ways
to approach the problem.
The first way is to have a writ-
ten policy on substance abuse in
advance. Any such policy should
either be developed by or reviewed
by legal counsel. The policy can be
included in an employment con-
tract, an employee manual or as a
stand-alone policy. In any case, it is
important that the employee read
and sign the policy. The policy
should clearly outline what the
practice will do if substance abuse
is suspected.
The second way comes after you
suspect there is a problem. That’s
when things can get complicated,
especially if no policy is in place.
Attorneys recommend you docu-
ment any unusual behavior or per-
formance problems you see, and
A M E R I C A N M E D I C A L N E W S A M E D N E W S . C O M J A N U A R Y 1 6 , 2 0 0 6
21
BusinessP R A C T I C E M A N A G E M E N T n P E R S O N A L F I N A N C E n T E C H N O L O G Y
UnitedHealth-PacifiCare deal approved, with conditions [ PAGE 27 ]
Dealing with an impaired employee or physician is a challenge any doctor’s office may face one day.
Establishing a policy on substance abuse and focusing on treatment instead of punitive action can help.
No practice
is immuneStory by Carrie Printz n Illustration by Chang Park
Continued on next page
SPOTTING A PROBLEM
Stephen Ross, MD, clinical assistant professor of psychiatry at New
York University School of Medicine, identifies red flags that should
cause suspicion of a substance abuse problem. These are excerpted from
the December 2003 Virtual Mentor, the AMA ethics journal
(http://www.ama-assn.org/ama/pub/category/11711.html).
Work-related symptoms
n Late to appointments; increased absences; unknown whereabouts
n Unusual rounding times
n Increase in patient complaints
n Increased secrecy
n Decrease in quality of care; careless decisions
n Incorrect charting or writing of prescriptions
n Decrease in productivity or efficiency
n Increased conflicts with colleagues
n Increased irritability, aggression
n Smell of alcohol; overt intoxication; needle marks
n Erratic job history
Problems at home
n Withdrawal from family, friends, and community
n Legal trouble (i.e., driving while under the influence)
n Increase in injuries
n Increase in medical problems and number of doctor’s visits
n Increased agitation and conflict
n Financial difficulties
n Deterioration of personal hygiene
n Depression, anxiety, mood instability](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-20-320.jpg)
![PAGE 21
3
Can we break it
down to provide
more context?
Federal statistics for this story are vast and
potentially brain-numbing. The treatment is
built on the concept: Are physicians experi-
encing what the numbers are reporting?
This feature story tackled the human side,
while the carefully curated collection of
data presented the numbers. To target our
primary care audience, the goal was to
quantify interesting aspects of their
dominant slice of the more than 1 billion
visits. This took diving deeper into the
source data to make relevant comparisons
and calculations. (The print spread contains
numerous graphics that are not included
here due to space limitations).
SEPTEMBER 4, 2006 AMEDNEWS.COM AMERICAN MEDICAL NEWS
28
Health&SciencePUBLIC HEALTH n CLINICAL ISSUES n PATIENTS
FDA-produced TV aims to boost patient safety [ PAGE 31 ]
A
re more patients streaming through
your office door today than 10 years
ago? Does every third person seem to
have hypertension? Does the waiting
room empty out in the summer and fill back up
again come fall? If so, you aren’t alone.
The Centers for Disease Control and Preven-
tion has charted these and other trends — in
some cases for more than 30 years — to provide a
statistical snapshot of ambulatory care. AMNews
asked several physicians how their practices
compared with study conclusions and found, for
the most part, the findings are on target.
The tally of outpatient office visits has reached
new heights, increasing at
a pace three times the rate
of population growth over
the past decade, according
to CDC figures. And the
agency’s “National Ambu-
latory Medical Care Sur-
vey,” released in June,
showed more than half of
those office visits, or
58.5%, were to primary
care offices. It’s fair to say,
then, that physicians who
work in these settings
have seen a burgeoning
amount of foot traffic.
That’s no surprise to
family physician Ayaz
Madraswalla, MD, who
has practiced in Storrs,
Conn., for 11 years. He is
one of five physicians in
an office where only two
are accepting new pa-
tients. “I had to close my
practice to new patients af-
ter three or four years,” he
said. “I had really maxed
out on how many patients
I could take.”
“We average 20 to 25 pa-
tients a day,” said Dr.
Madraswalla, who is also president of the Con-
necticut Academy of Family Physicians. “We
leave two emergency openings in each session —
morning and afternoon — and, by the end of the
day, I would say that everybody is full.”
“We are definitely seeing more patients,”
agreed Patricia Sereno, MD, a family physician
in Malden, Mass. “I think people are coming to
the doctor more often.” Chronic conditions such
as diabetes and hypertension are driving increas-
es, she said, as doctors step up monitoring efforts.
There are also more options. “We have more
medications to treat patients,” said Mark Keat-
S
S S RG
5%
10%
15%
20%
25%
30%
35%
January-March April-June July-September October-December
29.9%
29.1%
18.2%
22.8%
22.6%
25.8%
18.7%
32.9%
31.2%
15.6%
22.7%
30.5%
(Percentage of all office visits)
FOR EVERY VISIT
THERE IS A SEASON
Musculoskeletal symptoms
Respiratory symptoms
Psychological and mental disorders
MEDS NOT ALWAYS
INCLUDED
0 1 2 3 4 5 6 7 8
Medications provided or
prescribed per office visit
50,000
100,000
150,000
200,000
250,000
300,000
(Visits in the thousands)
Breaking down a billion visits
Physicians say the portrait of care
drawn by federal statistics reflects
what they see in their offices.
STORY BY SUSAN J. LANDERS
SOURCE: “NATIONAL AMBULATORY MEDICAL CARE SURVEY,” 2004 AND 1994 SUMMARY REPORTS, CDC/NATIONAL CENTER FOR HEALTH
STATISTICS, JUNE 2006 AND APRIL 1996
1,106,067
OFFICE VISITS: 910,857
ALL OTHERS: 195,210
n Primary care
532,420
n Medical specialty
202,006
n Surgical specialty
176,431
n Emergency
110,216
n Outpatient
84,994
(All numbers in thousands)
I
f you think you’re busier than ever and your office visits have
ballooned, you’re not alone. And you’re probably right. A new study
from the CDC found that of the billion-plus patient visits for ambulatory
care in 2004, the vast majority were at physician offices. And of these office
visits — some 910 million — 58.5% were to primary care physicians.
2004
910,857
1994
681,457
INCREASE
33.7%
DECADE OF
GROWTH
(Numbers in thousands)
Numbers in
thousands
% with primary
care doctor
OFFICE VISITS ALL PREVENTIVE CARE
FEMALE 535,541 99,694 90.1%
< 15 years 70,184 19,440 96.6%
15-24 years 45,232 15,991 97.2%
25-44 years 133,318 34,756 96.3%
45-64 years 152,319 18,932 78.9%
65-74 years 63,202 5,095 65.7%
75 years > 71,286 5,481 68.3%
MALE 375,316 47,308 81.2%
< 15 years 77,726 19,151 96.3%
15-24 years 25,361 3,521 87.0%
25-44 years 60,943 6,573 70.3%
45-64 years 111,784 11,506 74.2%
65-74 years 50,224 4,126 62.7%
75 years > 49,279 2,432 47.5%
TOTAL 910,857 147,002 87.2%
WHO’S COMING TO YOUR OFFICE
MEDS NOT ALWAYS
INCLUDED
0 1 2 3 4 5 6 7 8
Medications provided or
prescribed per office visit
50,000
100,000
150,000
200,000
250,000
300,000
(Visits in the thousands)
I
f you think you’re busier than ever and your office visits have
ballooned, you’re not alone. And you’re probably right. A new study
from the CDC found that of the billion-plus patient visits for ambulatory
care in 2004, the vast majority were at physician offices. And of these office
visits — some 910 million — 58.5% were to primary care physicians.
2004
910,857
1994
681,457
INCREASE
33.7%
DECADE OF
GROWTH
(Numbers in thousands)
Numbers in
thousands
% with primary
care doctor
OFFICE VISITS ALL PREVENTIVE CARE
FEMALE 535,541 99,694 90.1%
< 15 years 70,184 19,440 96.6%
15-24 years 45,232 15,991 97.2%
25-44 years 133,318 34,756 96.3%
45-64 years 152,319 18,932 78.9%
65-74 years 63,202 5,095 65.7%
75 years > 71,286 5,481 68.3%
MALE 375,316 47,308 81.2%
< 15 years 77,726 19,151 96.3%
15-24 years 25,361 3,521 87.0%
25-44 years 60,943 6,573 70.3%
45-64 years 111,784 11,506 74.2%
65-74 years 50,224 4,126 62.7%
75 years > 49,279 2,432 47.5%
TOTAL 910,857 147,002 87.2%
WHO’S COMING TO YOUR OFFICE](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-21-320.jpg)
![PAGE 22
3
Can we break it
down to provide
more context?
This graphic takes advantage of unique
findings from a study. To bring greater
context to this feature on talking
to patients about money, the graphic
presents quotes from survey
participants, putting a human touch on a
personal topic. (The printed graphic
also included results for physicians,
which are not represented here because
of size constraints). The story and anoth-
er graphic cover the “how-to” aspects,
while this graphic spells out the nature of
the problem with greater nuance.
AMERICAN MEDICAL NEWS AMEDNEWS.COM OCTOBER 16, 2006
23
BusinessPRACTICE MANAGEMENT n PERSONAL FINANCE n TECHNOLOGY
PRACTICE POINTERS: 4 ways to increase your patient base [ PAGE 25 ]
W
hen internist G. Caleb Alexan-
der, MD, an assistant professor
at the University of Chicago, was
finishing his residency in a
Pennsylvania hospital, he found it sur-
prising how infrequently physicians had
meaningful discussions with patients
about the cost of the clinical decisions be-
ing made on their behalf.
Dr. Alexander said he shrugged off the
initial observation because most patients
in the inpatient setting were too sick to
contemplate the cost of their medical
treatment. But he began to wonder what
happens in the outpatient setting as pa-
tients and physicians discuss a treatment
course.
“Patient communication [about mon-
ey] is important, yet it’s often neglected,”
Dr. Alexander said. “It’s not so surpris-
ing in the inpatient setting because pa-
tients are so sick, and there’s less willing-
ness to tolerate cost-quality tradeoffs
because the stakes are higher.”
But the stakes, financially speaking,
are going up in the outpatient setting as
well. As more patients enter their doc-
tors’ offices carrying high-deductible
health plans, often with attached health
savings accounts, there is a growing shift
in the mind-set. As they are assuming
more out-of-pocket expenses on their
own, patients are asking more from their
physicians about the cost of their own
health care, and whether a lower-cost
procedure might be a better idea. That
can be jarring for a physician duty-bound to provide the
best course of care, with cost often a secondary concern.
“This issue is a critically important one and there is a
woeful lack of attention being given to it,” said Nileen Ver-
beten, vice president of the California Medical Assn. Center
for Economic Services. “The profession as a whole is not
trained to think about that.”
Lingering questions about communication between pa-
tients and physicians led Dr. Alexander to plot a course of
action that studied how physicians talk to patients about
the cost of medical treatment.
His study, published in the August 2004 Journal of Inter-
nal Medicine, found that most physicians felt they didn’t
have enough time to include money conversations with pa-
tients in the exam room and that doctors felt uncomfortable
with the topic, broaching it only when necessary. Patients
also tended to be uncomfortable talking about money and
believed that bringing it up might compromise the quality
of their care.
What to do?
Robert Sade, MD, chair of the American Medical Associa-
tion’s Council on Ethical and Judicial Affairs, said there
aren’t many guidelines for physicians when it comes to talk-
ing money with patients.
Instead, Dr. Sade, a professor of surgery at the Medical
University of South Carolina, said the AMA’s Code of Ethics
indirectly prompts physicians to provide information to
help guide patients in their medical decisions.
“The physician’s responsibility is to discuss the situation
and make sure [patients] understand the medical value
of alternative treatments and relate those outcomes to
the cost, and, with the patient, decide what the bigger pic-
A delicate
balance
Here are five
things to remem-
ber when talking
to patients about
cost.
n Be sensitive to
your patient’s fi-
nancial needs by
creating an envi-
ronment in which
patients feel com-
fortable talking
about medical
costs.
n Be willing and
open to discuss
your patient’s fi-
nancial situation,
whether by gently
but firmly initiat-
ing the conversa-
tion at the appro-
priate time, such
as when writing a
prescription, or
taking the time to
discuss the issue if
the patient brings
it up.
n Be honest about
the cost of medical
procedures and be
ready to present
viable options to
the patient.
n Be attentive to
patient cues that
suggest financial
stress.
n Be aware that
your patient’s fi-
nancial situation
might affect the
ability to follow a
recommended
course of medical
treatment.
SOURCES: C. CALEB
ALEXANDER, MD,
ASSISTANT PROFESSOR,
UNIVERSITY OF CHICAGO;
GARY CORDINGLEY, MD,
NEUROLOGIST, ATHENS,
OHIO; WILLIAM ANDERECK,
MD, INTERNIST, SAN
FRANCISCO
Money
Talks
Paying for care can be a sensitive doctor-patient
discussion. Here is some advice for dealing with
those uncomfortable situations.
STORY BY JONATHAN G. BETHELY n ILLUSTRATION BY GRADY MCFERRIN
Continued on next page
Outside the comfort zone
It’s not easy for physicians and patients to discuss money. In a survey on the subject by C.
Caleb Alexander, MD, assistant professor at the University of Chicago, 133 internists and 484
patients from Midwestern academic and community practices identified some of the barriers.
Examples are taken from respondents’ comments. Respondents were allowed to name more
than one barrier.
FOR PATIENTS
BARRIER (FREQUENCY) EXAMPLE
Discomfort (19%) n “I didn't feel comfortable bringing up the issue.
n “I didn't know if it was normal”
n “Personal embarrassment”
Time (13%) n “They’re too busy”
n “From past experience, it’s not considered appropriate”
Physician lacked solution (11%) n “I thought that he wasn’t a part of it or that it
wouldn’t be helpful”
n “I didn’t know if it would make a difference”
Didn’t anticipate problem (11%) n “I didn’t know if my prescription was covered by
my insurance”
n “I didn’t think it was necessary”
Quality concerns (9%) n “For fear that they would give me a substitute that
wouldn’t work as well”
n “It might jeopardize my health”
Didn’t know doctor’s role (9%) n “Because you’re not sure if he has anything to
do with it”
n “Because from past experience, it’s not considered
appropriate”
Other (30%) n “Some of them may not know what the costs are”
n “Slipped my memory”
n “She hears it all day long”](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-22-320.jpg)
![PAGE 23
3
Can we break it
down to provide
more context?
While the story focuses on laws in Maryland and
North Carolina, the accompanying map gives the
piece a broader feel by providing national
context. Although most doctor readers aren’t
directly impacted by the two lawsuits
mentioned, the story notes that all but 19 states
have some kind of law or case law addressing
wrongful birth. The map allows the doctor to
quickly see if his or her state allows the claims,
does not allow the claims, or has no opinion on it.
n The top golf doctors say they play a
couple of times a week but have no
illusions about joining the PGA Tour.
DAMON ADAMS
AMNEWS STAFF
Ophthalmologist Dan Whipple, MD, readily admits
he’s no Tiger Woods.
“He was probably better as a 12-year-old than I
am now,” he jokes.
The physician, 44, also confesses that he’s not as
good as the PGA Tour’s 197th ranked golfer, a friend
he hit the links with recently. “He just killed me,”
said Dr. Whipple, of Avon, Ind., not bothering with
the gory details. “I couldn’t wait to get back to my
buddies to get my game back.”
For it is among his colleagues that Dr. Whipple is
on the leader board.
So says the August Golf Digest magazine, which
rates the physician as tied for 8th in the top golfing
doctors in America. As part of a special health sec-
tion, the 1.6-million circulation magazine ranked the
top 250 doctors on the fairways and greens.
Golf and medical associations were consulted, as
were doctors in the Castle Connolly annual guide,
America’s Top Doctors (4th Edition). Doctors listed
in regional magazines were considered, too. Only
practicing physicians made the cut, and the rank-
ings were compiled using the U.S. Golf Assn. Handi-
cap Index, a number based on a golfer’s ability and
course difficulty.
When told of how they fared, many on the maga-
zine’s list were as thrilled as hitting a hole in one. “I
remember one doctor saying, ‘This is the most ex-
citing thing that has happened to me since I gradu-
ated from medical school,’ ” said Golf Digest con-
tributing editor Lisa Furlong, who wrote the
rankings article.
At first, Steve Samuelson, MD, figured it was a
gag when told Golf Digest was on the line. Must be
one of his brothers playing a practical joke, he
thought. Turns out there’s nothing to snicker about
when Dr. Samuelson swaps his black bag for a golf
bag. He is tied for 4th, an honor not unnoticed by his
patients.
“They said, ‘No wonder I can’t get in to see you;
you’re out there golfing all the time.’ I just say,
‘Yeah, we’ll get you in,’ ” said Dr. Samuelson, an
ophthalmologist in Fremont, Neb.
Like most top golf docs, Dr. Samuelson has an
athletic past; he played for the golf team at the Uni-
versity of Nebraska at Kearney, where he was an
academic All-American. He won the 2003 Nebraska
Mid-Amateur Championship.
“I enjoy the competition. Most doctors have a
competitive streak in them,” he said.
California hematologist/oncologist Patricia Cor-
nett, MD, is the top female golfer and No. 7 overall
SEPTEMBER 4, 2006 AMEDNEWS.COM AMERICAN MEDICAL NEWS
Professional Issues
ETHICS FORUM: When can doctors stop taking new Medicare patients? [ PAGE 17 ]
HEALTH CARE LITIGATION n MEDICAL EDUCATION n ETHICS n PROFESSIONAL REGULATION
PLAYING UP TO PAR
Golf Digest’s ratings of the nation’s best golf-
ing doctors listed 15 orthopedic surgeons in
the Top 100, the most by any specialty. Urolo-
gists finished second, with eight making the
Top 100. Here are some tidbits the magazine
gathered by surveying 200 golfing docs:
87%have been asked for free medical
advice during a round of golf.
46%have treated an ill or injured
golfer on the course.
43%think sex the night before a
round can have a positive effect
on one’s golf game.
22%would try to keep an appointment
with Tiger Woods in a pro-am
at Pebble Beach even if they woke up with
heart attack symptoms.
10%say the pressure of a tough putt in
a tournament could be hazardous
to one’s health.
Among peers, Golf Digest says
these physicians rule the course
Among peers, Golf Digest says
these physicians rule the course
Leaders of the links
Continued on page 13
PHOTO BY GREG FOSTER
Douglas Hanzel, MD, a Savannah, Ga., pulmonary
specialist who garnered the top spot in Golf Digest’s
top golfing doctors list, enjoys golfing with his son.
Wrongful birth case crosses state lines
n The child was born in
Maryland, but a genetic test
was interpreted in North
Carolina. A court will decide
which state’s law applies.
AMY LYNN SORREL
AMNEWS STAFF
A Maryland couple alleges that if it
weren’t for the erroneous interpreta-
tion of a fetal test for cystic fibrosis by
two geneticists at North Carolina-
based Laboratory Corporation of
America, they would have aborted the
child who was born with the disease.
Karen and Scott Hood filed a
wrongful birth lawsuit against the
company, seeking to recover money to
cover the costs of caring for an ill
child. But they’ve run into a problem
that an increasing number of couples
could face: Maryland, where they live,
recognizes parents’ right to recover
damages for the wrongful birth of a
child; North Carolina, where the lab
performed the tests, does not.
Not surprisingly, the couple wants
Maryland’s law to apply; the company
wants North Carolina’s to apply.
In a preliminary ruling in June,
U.S. District Court Judge Catherine C.
Blake asked the Maryland Court of
Appeals, the state’s highest court, to
resolve the conflict. Oral arguments
are expected to take place in the fall.
“Indeed if a medical testing compa-
ny were only subject to the laws of the
state in which the actual testing was
conducted, and not the laws of the
state in which its patients were locat-
ed, medical testing companies would
have an incentive to locate in states
that provide the most protection to
the company and the least protection
to patients,” Blake wrote.
The decision, legal experts say,
could mean more litigation for doc-
tors if these cases are allowed to reach
across state lines.
“As genetic technologies improve
and we have more sophisticated kinds
of testing, the legal structures are
breaking down,” said attorney Susan
L. Crockin, a legal expert on reproduc-
tive genetics and a consultant to the
Genetics and Public Policy Center at
Johns Hopkins University. The center
studies human genetics and the relat-
ed ethical, legal and social concerns.
State high courts and federal court
decisions covering 25 states and the
District of Columbia have upheld
wrongful birth claims, according to a
2005 article Crockin authored for Re-
productive BioMedicine Online, an
independent international journal on
human conception.
Because not all states acknowledge
wrongful birth, “it’s inevitable that
we are going to have more issues
Continued on page 12
10
JUDICIAL REVIEW
Judges have been the ones to decide whether parents
can go forward with wrongful birth claims, with
state high court and federal court decisions
resulting in 25 states and the District of Columbia
recognizing claims, according to Reproductive
BioMedicine Online. Six states don’t allow wrongful
birth claims, and 19 have no case law.
n Allow wrongful birth claims
n Don’t allow wrongful birth claims
SOURCE: “REPRODUCTION, GENETICS AND THE LAW,” RBMONLINE, APRIL 14, 2005](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-23-320.jpg)
![PAGE 24
7 5
2
18
12
9
1
4
6
3
1
8
2 11
25
2
4
49
9
11
3
21
3
3
SICKENED BY SPINACH
The Centers for Disease Control and Prevention reports that 192 persons
were infected with E. coli O157:H7 during the outbreak. Among the ill
persons, 51% were hospitalized, 16% developed hemolytic-uremic
syndrome, and two died. Wisconsin, Ohio and Utah were the hardest hit.
REPORTED CASES BY STATE
0 1-4 5-9 10-14 15 or more
SOURCE: CENTERS FOR DISEASE CONTROL AND PREVENTION
3
Can we break it
down to provide
more context?
As demonstrated by this story, the best
way to explain a national trend is
usually with mapped data. It would be
difficult to clearly convey the
distribution of E. coli cases in text alone.
While the story focuses on the physician
role in tracking the outbreak, the map’s
increasing color density key gives
readers a quick sense of the areas most
impacted. The addition of the specific
numbers works well in this case,
because the figures are small and only
affect a portion of the country. Higher
numbers, or more numbers, would
overwhelm the presentation.
AMERICAN MEDICAL NEWS AMEDNEWS.COM OCTOBER 23/30, 2006
37
Health&SciencePUBLIC HEALTH n CLINICAL ISSUES n PATIENTS
CDC reports enough flu shots for everyone [ PAGE 40 ]
n The nation’s recent E. coli
experience shows how
physicians fit into the public
health continuum.
KATHLEEN PHALEN TOMASELLI
AMNEWS CORRESPONDENT
Last month, disease detectives pur-
sued a DNA fingerprint across 26
states, searching for clues to the
source of an unusually widespread
outbreak of Escherichia coli 0157:H7.
An early match to a bag of fresh
spinach in Colorado helped state and
federal epidemiologists trace the cul-
prit back to a California grower on
Sept. 29 — 15 days after the Food and
Drug Administration advised con-
sumers not to eat the leafy vegetable.
“This is not the first time molecu-
lar fingerprinting has helped track
outbreaks,” said Mel Kohn, MD, MPH,
Oregon’s state epidemiologist. “For
us, an astute epidemiologist picked up
a trend and zeroed in on spinach.
When we presented our five initial
cases to the Centers for Disease Con-
trol and Prevention, it matched infor-
mation from other states.”
The current outbreak, associated
with 192 reported cases, including 30
cases of hemolytic uremic syndrome,
98 hospitalizations and two deaths, is
not the first. There has been a long
history of E. coli outbreaks involving
leafy greens from the central Califor-
nia region.
“This is the 20th outbreak since
1995,” said Douglas Powell, PhD, asso-
ciate professor and scientific director
of the Food Safety Network at Kansas
State University in Manhattan. “For
example, in 1996 there was the Odwal-
la apple juice E. coli outbreak. In 2005
there was a national recall of Dole
bagged lettuce.”
While parallel laboratory and epi-
demiological investigations are cru-
cial in identifying the source of such
outbreaks, the hunt begins with the
patient and physician. Without physi-
cian involvement, early patterns and
clusters may go unnoticed, giving the
n Problems may stem from treatment.
Experts say a new study offers another
warning to use these drugs judiciously.
VICTORIA STAGG ELLIOTT
AMNEWS STAFF
Patients with chronic back injuries who become de-
pendent on opioids during the course of their treat-
ments use far more health care services and are less
likely to return to work than are those who do not
abuse these drugs, according to a study presented at
the North American Spine Society’s annual meet-
ing last month in Seattle.
“Don’t be afraid to use opioids early in the course
of the disease or for severe exacerbations,” said
Tom Mayer, MD, lead author and medical director
of the PRIDE, Productive Rehabilitation Institute of
Dallas for Ergonomics. “But with long-duration use,
there are significant risks.”
Dr. Mayer and his team followed 1,200 patients
who completed the institute’s rehabilitation pro-
gram. They had been treated for an average of a
year and a half before starting
the program, and 1.3% were
opioid-dependent before their
injuries. This number in-
creased to 14.3% during initial
treatment but prior to enter-
ing the program, which re-
quires participants to taper
from the medications.
Despite the fact that the pa-
tients all finished their reha-
bilitation off the medications, earlier dependence
clearly exacted a price. A year after finishing rehab,
those who were dependent were 2.8 times less likely
to have returned to work. They were also 2.1 times
more likely to have sought additional health care
services and 1.8 times more likely to have had addi-
tional surgeries.
“Opioid dependence disorder in these patients is
almost an entirely iatrogenic issue, and patients
may well have a poorer outcome,” said Dr. Mayer.
Experts praised this study for quantifying some
of the impact of opioid dependence among chronic
back pain patients and rein-
forcing the need for judicious
prescription drug use.
“The bottom line is that, so-
cioeconomically, individuals
who develop opioid depen-
dence do worse,” said Douglas
Paauw, MD, a general internist
and professor of medicine at
the University of Washington.
“And this really showed that
our interventions can help and they can harm.”
Classifying the disorder
While there was praise for this study, there were al-
so concerns about how these patients were classi-
fied in terms of opioid dependence disorder. Re-
searchers used DSM-IV criteria, but there is
significant agreement that this is not a very sensi-
tive way to detect the problem in patients legiti-
mately prescribed these medications.
“This is a good study with a large sample size,”
Opioid dependence linked to worse outcomes in back injury patients
Continued on page 39
7 5
2
18
12
9
1
4
6
3
1
8
2 11
25
2
4
49
9
11
3
21
3
3
Doctors play role in
tracking outbreak
Suspicious spinach
Continued on next page
Researchers suggest
that opioid use among
some pain patients may
reduce their motivation
to get better.
SICKENED BY SPINACH
The Centers for Disease Control and Prevention reports that 192 persons
were infected with E. coli O157:H7 during the outbreak. Among the ill
persons, 51% were hospitalized, 16% developed hemolytic-uremic
syndrome, and two died. Wisconsin, Ohio and Utah were the hardest hit.
REPORTED CASES BY STATE
0 1-4 5-9 10-14 15 or more
SOURCE: CENTERS FOR DISEASE CONTROL AND PREVENTION
PHOTO © VISUALS UNLIMITED/CORBIS
Escherichia coli serotype 0157:H7 is a
gram-negative rod-shaped bacterium
producing Shiga toxins.](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-24-320.jpg)
![PAGE 25
SOURCES: AMNEWS INTERVIEWS
AND MEDICAL SCHOOL WEB SITES
South America
Argentina UCSF
Bolivia UCSF
Brazil VAN
Ecuador UCSF, UMHS
Peru UWSM, VAN
Australia
Australia UWSM
Marshall Islands UWSM
New Zealand DAR
Asia
China STN, UCSF, UMHS, VAN
India VCOM, MTS, STN,
SUNY, UCSF, UWSM
Israel MTS
Japan UMHS
Qatar UPMC, COR
Russia VAN
Singapore DUK
Thailand SUNY, UCSF, UMHS
Tibet STN
Vietnam YALE
North America
Belize MSU, UCSF
Costa Rica UCSF
Dominican Republic VCOM
El Salvador VCOM, UCSF
Guatemala VCOM, MTS, STN
Honduras YALE
Mexico BAY, STN, UCSF, VAN
Nicaragua DAR, UCSF
Europe
Austria UMHS
Croatia UCSF
France UMHS
Ireland UPMC
Italy UPMC
Romania BAY
Sweden UMHS
Africa
Botswana BAY
Burkina Faso BAY
Cameroon UWSM
Eritrea YALE
Ghana UMHS, UWSM
Kenya IU, SUNY, UCSF
Lesotho BAY
Malawi BAY, MSU
Mali IOW
Nigeria ARK
Rwanda MTS
South Africa MTS, STN, YALE
Swaziland BAY
Tanzania DAR, UCSF
Uganda BAY, UCSF, YALE
Zambia VAN
Zimbabwe MSU
3
Can we break it
down to provide
more context?
The text in this story notes that 96 medical schools among the AAMC’s 125
members offer elective rotations. The map nicely details information about
which schools have set up programs where. This important context would
only bog the story down. Although the map does not detail all 96 medical
schools, it gives a good idea of the global reach that 18 of the schools have.
(In print, the map ran with a key explaining school names).
n Politicians in many states, though, are
forging ahead.
KEVIN B. O’REILLY
AMNEWS STAFF
Physician objections helped persuade Merck & Co.
Inc. to end its lobbying campaign for states to man-
date its new human papillomavirus vaccine, mar-
keted as Gardasil.
Merck did not respond to AMNews interview re-
quests by press time, but a company executive told
The New York Times that the mandate push was
counterproductive.
“Our goal is to reach as many females as possi-
ble,” Richard M. Haupt, MD, MPH, executive direc-
tor of medical affairs at the firm’s vaccine division
told the Times. “Right now, school requirements
and Merck’s involvement in that are being viewed
as a distraction to that goal.”
Joseph A. Bocchini, MD, chair of the American
Academy of Pediatrics’ Committee on Infectious
Diseases, said Merck did the right thing.
“The school mandate issue was changing the fo-
cus from the benefits of the vaccine to controversies
over whether mandates should be used,” Dr. Boc-
chini said.
Arthur Allen, author of Vaccine: The Story of
Medicine’s Greatest Lifesaver, said Merck
had little choice but to pull back. “Vaccina-
tion is a pretty fragile three-way agree-
ment between the vaccine makers, public health of-
ficials and the public,” he said. “If the public is
going south on it and public health is not into it,
you’re out there on your own, and that’s what was
happening to Merck.”
At press time, Texas state legislators were mov-
ing to rescind Republican Gov. Rick Perry’s Febru-
ary executive order mandating the cervical cancer
vaccine for 11- and 12-year-olds.
The Virginia General Assembly passed a re-
quirement, but Democratic Gov. Tim Kaine had not
yet taken action. Twenty other states were consid-
ering mandates, according to the National Confer-
ence of State Legislatures. u
T
hey bounced along the rutted
road to Eldoret, Kenya, with
their patient lying across the
SUV’s backseat. One team mem-
ber carried the woman, Ann, who was
wasted from AIDS, into the emergency de-
partment. It was 2004, and Sonali Sakaria,
MD, then a fourth-year medical student
from Indiana University School of Medi-
cine, walked alongside. She tried to not
gag on the stink of feces.
Medicine in a developing nation brings
a host of unexpected sights and smells, as
well as more significant challenges, such
as limited access to diagnostic tools like
x-rays. But for medical students, a two-
month stint in a developing nation can be
the highlight of their training.
“The patients were so appreciative,”
said Dr. Sakaria, now a second-year inter-
nal medicine resident at Emory Universi-
ty School of Medicine in Atlanta. “They
made you feel proud to be in medicine.”
U.S. medical schools such as Indiana Univer-
sity are making significant contributions to
health care worldwide and in the
process are giving medical students, res-
idents and practicing physicians the
chance to benefit personally and profes-
sionally as they share their expertise.
Ninety-six medical schools among the
125 members of the Assn. of American
Medical Colleges offer medical students elective
international rotations. At least half of the 23 os-
teopathic schools have overseas training. Data
from past years are scarce, but anecdotally med-
ical education leaders said there has been rapid
growth in such alliances in the past decade.
Most of these relationships are philanthropic,
like the IU-Kenya Partnership. A few are profit-
oriented. Regardless, U.S. medical students are
interested. Nearly 39% of U.S. medical students
studied in other countries in 2002, according to
the latest data from the AAMC, up
sharply from 20% in 2000 and 6% in 1982.
“The students recognize that it’s a
very small world we’re working in,” said
M. Brownell Anderson, the AAMC’s se-
nior associate vice president of medical
education.
The experiences deepen students’ sense of al-
truism and compassion, broaden understanding
of public health, increase cultural competence
and heighten awareness of the importance of
communication. It also leaves them more open to
volunteering in underserved communities, ac-
cording to “Expanding the Boundaries of Med-
ical Education: Evidence for Cross-Cultural Ex-
changes,” a review of 42 studies of cross-cultural
medical experiences in the Oct. 2003 supplement
of Academic Medicine.
Dr. Sakaria’s medical mission influenced her
career choice. She selected a residency at Emory
because of its strong infectious disease depart-
ment and connections with the Centers for Dis-
ease Control and Prevention.
EMPOWERING OTHERS
U.S. medical educators want to cultivate respons-
es similar to Dr. Sakaria’s, said Robert Einterz,
MD, associate dean of the IU-Kenya Partnership.
To create meaningful experiences for U.S. med-
icals students, there has to be a meaningful part-
nership with the other country, he said.
MARCH 12, 2007 AMEDNEWS.COM AMERICAN MEDICAL NEWS
10
Professional Issues
Physician-ethicist dissects “Ashley treatment” decision [ PAGE 14 ]
HEALTH CARE LITIGATION n MEDICAL EDUCATION n ETHICS n PROFESSIONAL REGULATION
Merck ends push for HPV vaccine mandate
Learning without
MORE U.S. MEDICAL SCHOOLS ARE
OFFERING OVERSEAS CLERKSHIPS, AND
STUDENTS ARE EAGER TO GO.
B RDERS
PHOTOS COURTESY OF UNIVERSITY OF MICHIGAN
University of Michigan undergrad Brandi Thompson (left photo) was one of 24 volunteer tutors with the Quito
Project in Equador last summer. Medical students Allan Peetz and Steven Gross were volunteers with Health In
Action, which aims to develop community-driven health care through education, prevention and medical care.
Continued on next page
STORY BY
MYRLE
CROASDALE](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-25-320.jpg)
![PAGE 26
State Year law Patient registry
took effect Yes No
Alaska 1999 X
California 1996 X
Colorado 2001 X
Hawaii 2000 X
Maine 1999 X
Montana 2004 X
Nevada 2001 X
Oregon 1998 X
Rhode Island 2006 X
Vermont 2004 X
Washington 1998 X
SOURCE: NATIONAL ORGANIZATION FOR THE REFORM OF
MARIJUANA LAWS
3
Can we break it
down to provide
more context?
This feature explores the medical marijuana
debate and that physicians say it’s time for
the federal government to allow studies on
the drug’s clinical benefits. To provide the
national picture, this graphic lists the 11
states that have legalized medical marijuana
and notes where they stand on patient
registries. Geographic distribution is less
important with this content, so the concise
table makes access to the information
easiest. Because every relevant state is
accounted for, the graphic adds context to
this national story.
Frank H. Lucido, MD, a family
physician in Berkeley, Calif., has
recommended cannibis to a
patient for the treatment of
chronic pain.
I
f there were a drug with the poten-
tial to alleviate the pain and suffer-
ing of the sickest patients, for
whom all other treatments have
failed, should patients be allowed to
use it? Should independent medical re-
searchers be able to study it? Should physi-
cians be able to prescribe it?
What if that drug was marijuana?
Frustrated doctors and scientists say
that in marijuana’s case, the federal gov-
ernment’s answer is no.
Classified by the Drug Enforcement Ad-
ministration as a Schedule I controlled sub-
stance, cannabis can be researched as a
medicine only with federal approval. The
National Institute on Drug Abuse controls
the supply for U.S. studies.
Although physicians debate the likely
value of marijuana as medicine, they agree
that, unlike other drugs with therapeutic
potential, the government has taken a con-
trolling interest in it. This has hindered the
research necessary to find out whether cannabis
can effectively help patients with serious medical
conditions.
The Food and Drug Administration, DEA and
NIDA declined to comment. But the FDA in April
issued a statement reiterating its position that
“no sound scientific studies support medical use
of marijuana for treatment in the United States.”
Still, states continue to pass laws allowing its
use with a doctor’s recommendation, in spite of
an overriding federal ban on the drug’s prescrip-
tion and use. The disconnect between federal and
state laws poses risks to both doctors and pa-
tients, physicians say. It’s time, they add, to ex-
pand research and resolve the issue so they can
exercise control in the care of patients who seek
marijuana for medicinal purposes.
Dangers for doctors and patients
“It would be helpful if we did the standard rigor-
ous studies needed instead of having to wander in
the dark,” said California Medical Assn. Presi-
dent Michael J. Sexton, MD. California in 1996 be-
came the first state to make it legal for patients
with specific, debilitating illnesses to grow and
possess small amounts of marijuana with a doc-
tor’s recommendation. Rhode Island’s passage of
a law in January brought the number of states al-
lowing medical marijuana to 11.
In those states, most medical
societies, like the CMA, have
not taken a position on the
statutes or whether the drug
has medicinal value. Organized
medicine’s main concern has
been protecting the doctor-pa-
tient relationship and doctors’
right to openly discuss the sub-
stance as a treatment option
without fear of prosecution or
loss of their medical licenses.
In 2003, doctors won a small
victory when the U.S. Supreme
Court declined to change a 9th
U.S. Circuit Court of Appeals
decision reinforcing this priva-
cy, even when it involves con-
versations about cannabis.
However, patients are left un-
protected because the court in
2005 concluded that, regardless
of state laws, the federal govern-
ment has the right to arrest pa-
tients for marijuana possession.
Frank H. Lucido, MD, treat-
ed Angel McClary Raich, one of
the people who brought the
case that was decided last year.
He recommended cannabis to
alleviate Raich’s chronic pain
caused by an inoperable brain
tumor and severe scoliosis,
among other ailments.
The court’s ruling in Raich’s
case could also put physicians
in a precarious situation, Dr.
Lucido warned. When dis-
cussing the substance, doctors
must be cautious “not to be per-
ceived as aiding or abetting pa-
tients in obtaining cannabis,”
he said.
A family physician in Berke-
ley, Calif., Dr. Lucido said he
was investigated by the state
medical board in 2002 for rec-
ommending marijuana to a patient, although the
case was closed with no charges filed. Since then,
he has advocated and testified for other doctors
investigated by state authorities despite Califor-
nia’s medical marijuana law.
Anecdotally, doctors say, the DEA has not pur-
sued them or patients. Nonetheless, risks remain.
Some of those dangers aren’t legal but medical.
“It makes physicians uneasy that they can’t su-
pervise or have some sort of control over what
their patients are doing,” said Lynn Parry, MD,
president-elect of the Colorado Medical Society. A
neurologist, Dr. Parry said she has recommended
medicinal marijuana to patients with chronic
AMERICAN MEDICAL NEWS AMEDNEWS.COM JULY 10, 2006
5
Physicians push to delay move to new ICD code set [ PAGE 8 ]
MEDICARE / MEDICAID n LEGISLATION AND REGULATION n NATIONAL HEALTH POLICY
Government&Medicine
Physicians say it’s time for the federal government
to allow studies to put to rest the question of
whether the drug has clinical benefits.
Story by Amy Lynn Sorrel | Photograph by Victor James Blue
Arrested
development
Medical marijuana
Continued on next page
State action
In spite of federal law prohibiting the use and
prescription of cannabis, a growing number
of states continue to pass measures legalizing
marijuana for medicinal purposes with a
doctor’s recommendation. Some laws have
also established state-run patient registries
that issue identification cards to people qual-
ifying to use the drug for medical reasons.](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-26-320.jpg)
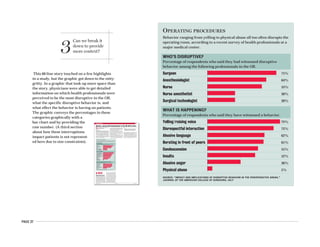
![PAGE 28
3
Can we break it
down to provide
more context?
The number of uninsured Americans creeps upward each year, and our
challenge is to engage the reader with a story that’s not much different than it
was the year before. There is a ton of data, but we’ve only recently found our
stride in presenting it. Of the several graphics with this page 1 story, this one is
the most striking because it is the most direct. By using raw numbers and four
distinctions, we plotted people instead of percentages. Other graphics got into
state-by-state comparisons and breakdown by age. This chart showed readers
that, despite the high rate of uninsured among various races and levels of em-
ployment, their next uninsured patient will likely be white or working full-time.
n The increase means more
patients will delay needed
care and be sicker when they do
come in, doctors predict.
GERI ASTON
AMNEWS STAFF
The number of uninsured Americans
grew by 1.3 million last year, mainly
due to the loss of employer-based cover-
age, new U.S. Census Bureau figures
show. Physicians said the news exacer-
bates their frustrations over the human
toll of the problem and the financial
strain it places on their practices.
The 46.6 million people who lack cov-
erage “don’t access care in a timely
manner,” said AMA Trustee Ardis D.
Hoven, MD, an internal medicine and
infectious disease specialist in Lexington, Ky.
The first thing uninsured patients skimp on is preven-
tive care, physicians said. “They think, ‘I don’t have insur-
ance so I can’t go to the doctor to get a Pap smear, a mam-
mogram, a colonoscopy,’ ” Dr. Hoven said.
Mark Macumber, MD, sees the problem’s impact every
day. He doesn’t accept insurance and
charges a flat $40 fee for office visits. Vir-
tually all of the patients at his two prac-
tices, one in Chicago and one in nearby
Berwyn, Ill., lack health coverage.
“I see some very scary things,” said
Dr. Macumber, an assistant professor of
family medicine at Northwestern Uni-
versity. “I see fractures, and people have
taken care of it themselves.”
Many uninsured patients are work-
ing poor, physicians said. They make too
much to qualify for Medicaid but too lit-
tle to afford insurance. Of the 37.8 mil-
lion people of working age who lacked
insurance in 2005, 27.3 million worked at
some point that year, according to the
Census Bureau figures, which approxi-
mate the number of people uninsured at
some point in the year. The number of
uninsured full-time workers grew from 20.5 million in 2004
to 21.5 million in 2005.
“When people think of the uninsured, they have a cer-
tain picture in their head, and it’s wrong,” Dr. Macumber
said. They aren’t totally impoverished people who can ac-
n Physicians say effective
communication boosts their
self-confidence, eases
interactions with colleagues and
improves patient care.
MYRLE CROASDALE
AMNEWS STAFF
Psychiatrist Fabien Tremeau, MD,
originally from France, no longer has
to repeat himself to be understood.
He credits professional coaching
with strengthening his American pro-
nunciation, leaving him with just a
mild French accent.
International medical graduates
such as Dr. Tremeau are among myri-
ad immigrants working in the United
States who find clear communication
crucial to their work. For physicians,
there’s an added urgency, because a
patient’s health and life may be at
stake.
One out of every four practicing
physicians in the United States is an
IMG, though there are no data on how
many speak English as a second lan-
guage. Nevertheless, as the number of
IMGs rises, anecdotal information
shows that whether it’s to improve pa-
tient interactions or to boost their
own self-confidence, there are more
doctors taking steps to tone down
their accents. They’re turning to
speech experts and dedicating an
hour or more a week for 12 weeks
and longer to polish their American
pronunciation.
Dr. Tremeau, who’s been in the
United States for 11 years, decided to
get formal speech training when he
realized he was no longer making
headway on his own. “[My accent]
wasn’t too much of a problem, but
there were times I was not sure how to
pronounce words. Sometimes I had to
repeat myself,” Dr. Tremeau said.
He also found that his accent could
www.amednews.com
AMERICAN MEDICAL NEWS
515 NORTH STATE
CHICAGO, IL 60610
★ ★ ★
CLASSIFIED ADVERTISING – PAGES 29-30
September 18, 2006
VOLUME 49 n NUMBER 35American Medical
Exporting patients
Lured by cheaper health care
overseas, payers increasingly
are offering patients the option
to go outside the United States
for certain procedures.
In Business, page 16
Mich. high court: Doctor
can sue over peer review
Professional Issues, page 9
First deadline for new
paper claim form
Business, page 21
Easing med student debt
Opinion, page 23
Photo exhibit explores
the intersection of
biology and art
Health & Science, page 27
Medicare takes a
payment holiday
Physician reimbursements
will be delayed so Medicare
can meet a spending target by
shifting $5 billion to the next
fiscal year. Doctors will get
paid, but don’t expect late fees.
In Government, page 5
Treating medically
unexplained woes
Sometimes patients have pain
and discomfort without signs
of a treatable disorder. Several
studies offer suggestions on
addressing the symptoms.
In Health & Science, page 26
Uninsured climb to 46.6 million
ANOTHER YEAR,
ANOTHER MILLION
The number of uninsured
Americans has marched
upward annually.
2005 46.6 million
2004 45.3 million
2003 45.0 million
2002 43.6 million
2001 41.2 million
NOTE: 2004 FIGURE REVISED AFTER
THE 2004 REPORT WAS RELEASED.
SOURCE: U.S. CENSUS BUREAU,
AUGUST
Accent on clarity
Doctors seek classes to Americanize their speech
Continued on page 4
Continued on next page
WHAT DID YOU SAY?
Non-native English speakers
can stumble over the pronuncia-
tions of words, which can be
especially problematic for
potential sound-alikes.
Pronunciations
n E. coli (ee-koh-lai)
n Influenza (in-flu-en-zah)
n Pneumonia (nu-moh-ni-ah)
n Amoxicillin (a-mak-sa-ci-lin)
n Ciprofloxacin (si-proh-flahks-
ah-sin)
n Imipenem (i-mee-peh-nim)
n Piperacillin (peh-pir-ah-si-lin)
n Tetracycline (te-trah-sai-
kleen)
Easily confused
n Bleeding, breathing
n Breast, breath
n Eyes, ice
n Knees, niece
SOURCES: WILLIAM BEAUMONT HOSPITAL’S
SPEECH & LANGUAGE PATHOLOGY DEPT.
ROYAL OAKS, MICH,; EXECUTIVEXPRESSION,
SHERMAN OAKS, CALIF.
Less than
$25,000
$25,000 -
$49,999
$50,000 -
$74,999
No high school
diploma
Some college,
no degree
Bachelor’s
degree or
beyond
Full time
Hispanic
AsianWhite, not
Hispanic
Part time
30
million
20
million
10
million
BY EDUCATION BY WORK EXPERIENCE
$75,000
or more
Did not
work
Counting the uninsured
Black
BY HOUSEHOLD INCOMEBY RACE
Associate’s
degree
Nearly 14.6 million people in
families earning less than
$25,000 lack insurance,
compared with 8.7 million
uninsured in families
earning $75,000 or more.
About 4.6 million people
with bachelor’s degrees or
beyond have no coverage,
compared with 14.1 million
who have only high school
degrees.
Almost 21.5 million full-time
workers were uninsured.
Most uninsured Americans,
22.1 million, are non-Hispan-
ic whites. The second largest
group, at 14.1 million, are
Hispanics.
High school
grad only](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-28-320.jpg)
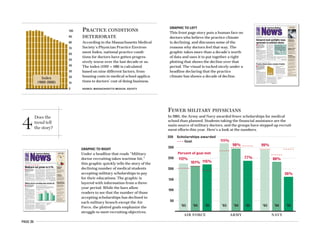
![PAGE 30
Based on a report about drug use, this
graphic offers comparisons while
maintaining its most important aspect
for the story: Trend. The story addresses
a range of findings in the report, while
this graphic focuses on three age groups.
In the layered graphic, it’s clearly shown
both how drug use is declining among
12- to 17-year-olds and how this compares
with other age groups. Another easy
comparison comes with the dashed line
representing the overall rate for people
older than 12.
n The medicine decreases cancer risk
while boosting cardiovascular disease
risk. Researchers are hopeful about the
future of chemoprevention of carcinoma.
VICTORIA STAGG ELLIOTT
AMNEWS STAFF
In September 2004, preliminary trial data were re-
leased suggesting that long-term use of COX-2 in-
hibitors brought an increased cardiovascular risk.
The finding made a big splash and ultimately led
to the dislodging of this drug class from the best-
seller list.
Now, two years later, the research question these
projects were designed to answer — whether the
COX-2s offer protection from certain cancers — has
been solved. These drugs do reduce the chance of
colorectal polyps in patients who have a history of
them, but the price of this prevention is a dramati-
cally increased risk of heart and vascular disease,
according to a pair of studies published in the New
England Journal of Medicine last month. The trials
randomized just over 3,500 patients to various
dosages of celecoxib (Celebrex) or placebo.
A related paper, this one published in the August
online edition of Gastroenterology and expected
in print in December, involved patients receiving
25 mg of rofecoxib (Vioxx) and reached similar
conclusions.
“The clear message is that COX-2 inhibitors pre-
vent colon polyps, and the effect is fairly substan-
tial,” said Curt Furberg, MD, PhD, professor of pub-
lic health sciences who participated in the Food and
Drug Administration advisory committee meetings
regarding safety issues related to these drugs. “But
that’s just one effect.”
An editorial, also in the August New England
Journal of Medicine, concluded that the dream of
using currently available COX-2 inhibitor medica-
tions for cancer prevention in the general popula-
tion is effectively dead. The burden of cardiovascu-
lar disease associated with their use is too great. Al-
so, although this regimen was proven to reduce
polyps that can lead to colorectal cancer, it has yet
to be shown to prevent actual cancers.
“The risk far exceeds the benefits,” said Bruce
Psaty, MD, PhD, the editorial’s lead author and a
SEPTEMBER 25, 2006 AMEDNEWS.COM AMERICAN MEDICAL NEWS
30
Health&SciencePUBLIC HEALTH n CLINICAL ISSUES n PATIENTS
CDC agreement gives access to flu virus fingerprints [ PAGE 33 ]
n An annual federal report on
drug, alcohol and tobacco
use also found that 71.5 million
Americans were current users
of a tobacco product.
SUSAN J. LANDERS
AMNEWS STAFF
Washington To paraphrase the rock
band The Who, the kids appear to be
all right. Or at least doing better. But
what about the grown-ups?
A large national survey shows that
while illicit drug use has dropped
among 12- to 17-year-olds, it has in-
creased among baby boomers and is
still high among young adults.
The results of the 2005 National
Survey on Drug Use and Health sug-
gest a change for the better among
young people but a resistance to
change in those old enough to be their
parents and even grandparents.
Illicit drug use among 12- to 17-
year-olds dropped from 11.6% in 2002
to 9.9% last year. That means that
367,000 fewer young people reported
using any illegal drug in the month
before they were queried.
The news was welcomed by White
House and federal agency officials
who released the report on Sept. 7
while also launching National Alcohol
and Drug Addiction Recovery month
to promote drug treatment.
“Teens ages 12 to 17 are signaling a
positive change in behavior,” said
John P. Walters, director of the White
House Office of National Drug Control
Policy.
“Kids in this country are making
better choices. I’m proud of them,”
agreed Assistant Surgeon General Er-
ic B. Broderick, DDS, MPH, who is al-
so acting deputy administrator for the
Substance Abuse and Mental Health
Services Administration, the agency
that administers the survey.
“We first saw this shift toward
healthier decisions when rates of to-
Drug use drops for teenagers
but remains higher for adults
Good news and bad news about COX-2s
THE RISE AND FALL OF COX-2 INHIBITORS
The Food and Drug Administration approved Celebrex (celecoxib) in 1998, Vioxx (rofecoxib) in
1999 and Bextra (valdecoxib) in 2001. With them came hopes for preventive powers. But risks, too,
soon emerged. Some key dates:
NOV. 23, 2000: Vioxx GI Outcomes Research
trial results published in the New England
Journal of Medicine indicate that arthritis pa-
tients who take rofecoxib have fewer gastroin-
testinal adverse events than those who take
naproxen. Cardiovascular risk appears similar.
AUG. 22, 2001: A special communication in the
Journal of the American Medical Association
notes a possible increased cardiovascular risk
associated with use of COX-2 inhibitors.
APRIL 11, 2002: Information about possible
increased cardiovascular risk added to the
label of rofecoxib.
SEPT. 30, 2004: Merck & Co. withdraws
rofecoxib from the market after data from trials
regarding its use to prevent colorectal polyps
and cancer confirm a significant increased
cardiovascular disease risk.
DEC. 9, 2004: Cardiovascular risk and severe
skin reaction warnings are added to the label
of valdecoxib.
DEC. 17, 2004: The National Cancer Institute
halts a study of celecoxib as a possible colon
polyp preventive because of an increase in
cardiovascular events among participants.
APRIL 7, 2005: Valdecoxib is withdrawn from
the market. Additional warnings about
cardiovascular risk are added to the label of
celecoxib.
AUG. 31, 2006: Two studies published in
New England Journal of Medicine confirm that
COX-2 inhibitors prevent colorectal polyps
but significantly increase the risk of
cardiovascular disease.
Continued on next page
WHO’S USING
The National Survey on Drug Use and Health reported that during 2005,
an estimated 19.7 million Americans age 12 or older were current drug
users. This represents approximately 8.1% of that population.
SOURCE: THE 2005 NATIONAL SURVEY ON DRUG USE AND HEALTH: NATIONAL FINDINGS, NATIONAL
INSTITUTE ON DRUG ABUSE, SEPTEMBERContinued on page 32
12-17 18-25 26 AND OLDER
25%
20%
15%
10%
5%
8.1%
Overall rate
for people older
than 12 (2005)
11.6%
11.2%
9.9%
Percentage of illicit drug use during
the previous month by age group
10.6%
20.2% 20.3%
19.4%
20.1%
5.8% 5.6% 5.5%
5.8%
2002
2003
2004
2005
4
Does the
trend tell
the story?
WHO’S USING
The National Survey on Drug Use and Health reported that during 2005,
an estimated 19.7 million Americans age 12 or older were current drug
users. This represents approximately 8.1% of that population.
SOURCE: THE 2005 NATIONAL SURVEY ON DRUG USE AND HEALTH: NATIONAL FINDINGS, NATIONAL
INSTITUTE ON DRUG ABUSE, SEPTEMBER
12-17 18-25 26 AND OLDER
25%
20%
15%
10%
5%
8.1%
Overall rate
for people older
than 12 (2005)
11.6%
11.2%
9.9%
Percentage of illicit drug use during
the previous month by age group
10.6%
20.2% 20.3%
19.4%
20.1%
5.8% 5.6% 5.5%
5.8%
2002
2003
2004
2005](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-30-320.jpg)
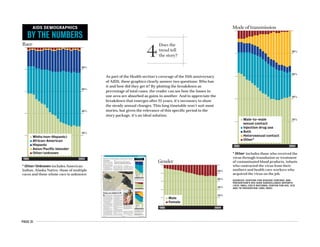
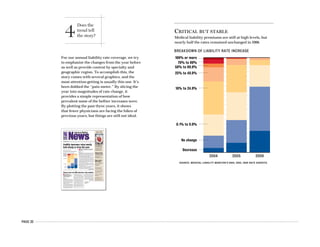
![PAGE 33
TORT REFORM IN ACTION
Insurers say tort reform has helped
stabilize medical liability rates,
although the laws’ uncertain staying
power leaves a question as to whether
the steady rates will continue. Here is
a look at the average premiums
internists paid between 2001 and 2006
in some states with tort reform, based
on insurer reports to Medical Liability
Monitor.
FLORIDA: Passed a $500,000 cap on
noneconomic damages in 2003 that
increases to $1 million under certain
circumstances. Passed a limit on
attorneys’ fees in 2004, which the state
Supreme Court in September said
attorneys can have patients sign a
form to waive.
TEXAS: Passed a $250,000 cap on
noneconomic damages in 2003, with
a $750,000 ceiling for multiple defendants.
The limit was approved as a
constitutional amendment, making
it more difficult to overturn in court.
LOUISIANA: Passed a $500,000 cap on
noneconomic damages in 1975. A state
appeals court overturned the cap in
September, ruling that the dollar amount
was too low. The case is headed to the
state Supreme Court.
CALIFORNIA: Passed a $250,000 cap on
noneconomic damages in 1975 that still
stands.
WISCONSIN: Passed a $350,000 cap on
noneconomic damages in 1995. The state
Supreme Court overturned the cap in
2005, when it stood at $445,775 adjusted
for inflation. Gov. Jim Doyle in March
approved a higher cap of $750,000.
’01
$5K
$10K
$15K
$20K
$25K
$30K
$35K
$40K
$45K
LIABILITY PREMIUM
’02 ’03 ’04 ’05 ’06
SOURCE: AMERICAN MEDICAL ASSOCIATION; AN AMNEWS
ANALYSIS OF MEDICAL LIABILITY MONITOR 2001 THROUGH
2006 RATE SURVEYS.
This is another of our graphics for the
liability rate coverage. To draw attention to
the impact of tort reform, we plotted the rate
for five states over a six-year period. Marginalia
adds another layer of information by highlighting
each state’s policies and caps. The plotting
encourages comparisons between states and
lends drama to the vast difference between rates
in Florida and those in Wisconsin. This graphic
works well with the others in the package
because it most directly addresses tort reform
while the others spell out the broader context.
LOCATION HELPS DICTATE PREMIUMS
Physicians in large metropolitan areas pay some of the highest medical liability insurance premiums in the nation. Below is a summary of the highest and
lowest reported rates for three specialties as of July 1. Companies reported their data based on annual rates for specific mature claims-made policies with
limits of $1 million/$3 million. The rates do not reflect credits, debits or dividends. The rankings are by state, county or city.
2005 2006 CHANGE
Florida (Dade) $74,855 $74,855 0%
Illinois (Cook) $65,887 $65,887 0%
Michigan (Wayne) $49,386 $48,041 -2.7%
Ohio (Cuyahoga, Lorain) $43,416 $43,192 -0.5%
Connecticut $34,700 $34,700 0%
Florida (Dade) $299,420 $299,420 0%
Illinois (Cook) $212,176 $212,176 0%
Michigan (Wayne) $162,623 $162,623 0%
Ohio (Cuyahoga, Lorain) $158,634 $160,162 1.0%
Missouri (Kansas City) $132,314 $132,314 0%
Florida (Dade) $299,420 $299,420 0%
Illinois (Cook) $266,349 $266,349 0%
Ohio (Cuyahoga, Lorain) $187,858 $194,293 3.4%
Maryland (Baltimore city) $157,524 $176,978 12.3%
New Jersey $146,267 $171,199 17.0%
2005 2006 CHANGE
Minnesota $3,375 $3,375 0%
South Dakota $3,697 $3,697 0%
Idaho $3,770 $3,770 0%
Nebraska $3,572 $4,548 27.3%
Wisconsin $5,147 $5,147 0%
Minnesota $11,306 $11,306 0%
South Dakota $12,569 $12,569 0%
Idaho $14,514 $14,514 0%
Nebraska $12,144 $17,328 42.7%
Wisconsin $18,015 $18,015 0%
Idaho $19,320 $19,320 0%
Minnesota $19,643 $19,643 0%
South Dakota $21,072 $21,072 0%
Wisconsin $23,677 $23,677 0%
Nebraska $17,144 $25,559 49.1%
AMERICAN MEDICAL NEWS (ISSN 0001-1843)
IS PUBLISHED WEEKLY, EXCEPT FOR 4
COMBINED ISSUES IN MONTHS WITH 5
MONDAYS, BY THE AMERICAN MEDICAL
ASSOCIATION, 515 N. STATE ST., CHICAGO, IL
60610. COPYRIGHT 2006 BY THE AMERICAN
MEDICAL ASSOCIATION. PRINTED IN THE USA.
American Medical News VOLUME 49 n NUMBER 46
American Medical News is published by the AMA and is intended to serve as a credible forum for information affecting
physicians and their practices. The contents of articles and the opinions expressed in AMNews are not necessarily endorsed
by the AMA.
DECEMBER 11, 2006 AMEDNEWS.COM AMERICAN MEDICAL NEWS
2 Cover Stories
TORT REFORM IN ACTION
Insurers say tort reform has helped
stabilize medical liability rates,
although the laws’ uncertain staying
power leaves a question as to whether
the steady rates will continue. Here is
a look at the average premiums
internists paid between 2001 and 2006
in some states with tort reform, based
on insurer reports to Medical Liability
Monitor.
FLORIDA: Passed a $500,000 cap on
noneconomic damages in 2003 that
increases to $1 million under certain
circumstances. Passed a limit on
attorneys’ fees in 2004, which the state
Supreme Court in September said
attorneys can have patients sign a
form to waive.
TEXAS: Passed a $250,000 cap on
noneconomic damages in 2003, with
a $750,000 ceiling for multiple defendants.
The limit was approved as a
constitutional amendment, making
it more difficult to overturn in court.
LOUISIANA: Passed a $500,000 cap on
noneconomic damages in 1975. A state
appeals court overturned the cap in
September, ruling that the dollar amount
was too low. The case is headed to the
state Supreme Court.
CALIFORNIA: Passed a $250,000 cap on
noneconomic damages in 1975 that still
stands.
WISCONSIN: Passed a $350,000 cap on
noneconomic damages in 1995. The state
Supreme Court overturned the cap in
2005, when it stood at $445,775 adjusted
for inflation. Gov. Jim Doyle in March
approved a higher cap of $750,000.
rates were cut, more than double the
number in 2005.
But doctors and insurers say early
signs of a better market for physicians
could be short-lived.
“The frequency of claims has really
leveled off, maybe even declining in
some places, like Texas. But the long-
term rise in the severity [of jury
awards] is still with us,” and might
warrant future rate hikes so that in-
surers can keep up with costs, said
Lawrence E. Smarr, president of the
Physician Insurers Assn. of America,
a trade group of medical liability com-
panies owned or operated by doctors.
More than 90% of firms responding
to the Monitor’s survey said rates are
stabilizing, up from 81% in 2005. None
believed “large increases” are neces-
sary, down from 6.3% last year. But
that would change if patients begin fil-
ing more lawsuits, insurers noted.
Litigation costs also continue to
drive up insurance prices, making the
future uncertain, doctors and insur-
ers say. A first-time report by the
Ohio Dept. of Insurance showed that
80% of the 5,051 claims closed in 2005
resulted in no payment. But nearly
92% of the claims incurred defense ex-
penses, totaling $113 million, or about
$24,000 per case.
“The trend of [rate] increases has
flattened,” said Ohio State Medical
Assn. Executive Director D. Brent
Mulgrew, “but we’re still paying an
awful lot of money for this system.”
The questionable staying power of
tort reform also has insurers’ opti-
mism waning. According to the Moni-
tor’s survey, 60% of companies in
states that passed reforms in the past
year said they had concerns about the
laws’ constitutionality.
Several recent state court rulings
have not been friendly to doctors. A
court decision led Wisconsin to up its
cap to $750,000. In Louisiana, the long-
time cap is up in the air, with the state
Supreme Court set to hear an appeal
of a September lower court ruling that
found the $500,000 cap too low.
Hopes of tort reform on a national
level are nearly nonexistent among
insurers. A single firm told Monitor
surveyors that tort reform would
come out of Congress, compared with
21% saying that last year.
Still, the survey continues to show
the direct results of significant tort re-
forms, the AMA’s Dr. Plested said.
For example, Texas voters in 2003
passed a $250,000 cap as a constitution-
al amendment, making it difficult for a
court to overturn. Texas Medical Lia-
bility Trust, which insures nearly half
of the doctors in the state, cut rates by
5% this year and has slashed them an
average of 29.5% since the law took ef-
fect, the Monitor report states.
In Illinois, Harold L. Jensen, MD,
chair of the physician-owned ISMIE
Mutual Insurance Co., said the com-
pany cut rates by an average of 5.2%
this year, due to a “halo effect” after
passage of a $500,000 cap in 2005. Still,
the state came in a close second for
the highest rates in the nation, the
Monitor’s survey shows.
“It’s looking better,” Dr. Jensen
said. “But it took us a long time to spi-
ral into the mess we’re in, and to be-
lieve we’re going to pull out in six
months to a year is not realistic.” u ’01
$5K
$10K
$15K
$20K
$25K
$30K
$35K
$40K
$45K
LIABILITY PREMIUM
’02 ’03 ’04 ’05 ’06
SOURCE: AMERICAN MEDICAL ASSOCIATION; AN AMNEWS
ANALYSIS OF MEDICAL LIABILITY MONITOR 2001 THROUGH
2006 RATE SURVEYS.
Continued from preceding page
Liability insurance rates mostly
hold steady or drop this year
SOURCE: MEDICAL LIABILITY MONITOR 2006 RATE SURVEY
LOWEST RATESHIGHEST RATES
Internists
General
surgeons
Ob-gyns
4
Does the
trend tell
the story?](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-33-320.jpg)
![PAGE 34
The feature discusses the need for a modern
emergency department and presents some of
the features it would include. The floor plan
and rendering bring the words to life. Floor
plans show the before and after of how walls
can be moved to accommodate more
patients. A rendering illustrates how the
hospital would be laid out, with a public
drive covered by a blast barrier, the secured
drop-off concourse and other unique aspects
of the building. (Not all renderings from
print are shown due to size constraints.)
AMERICAN MEDICAL NEWS AMEDNEWS.COM MARCH 5, 2007
5
Judge allows challenge to conscience clause over abortion to go ahead [ PAGE 7 ]
MEDICARE / MEDICAID n LEGISLATION AND REGULATION n NATIONAL HEALTH POLICY
Government&Medicine
By the time doctors realize the assault ex-
posed some victims to a deadly communicable
disease, hundreds more patients and medical
personnel have been infected. Entire hospitals
are declared quarantine zones.
Just when physicians think the situation
couldn’t possibly get worse, the terrorists launch
their second wave of attacks. Using truck bombs
to target emergency departments, the assailants
push several facilities past the point of total loss
and ensure the system’s complete breakdown.
Such a situation might seem hopeless, but
some physicians think at least one of the D.C.
area’s EDs can be modernized so it remains func-
tional and helps hold the system together amid
any disaster — natural or man-made.
ER One would be the nation’s first civilian
“all-risks-ready” emergency department. Wash-
ington Hospital Center, with the leadership of its
emergency department chair, Mark S. Smith,
MD, is planning to build the facility on its cam-
pus about two miles from the U.S. Capitol.
During an average day, it would operate as a
typical fully functioning ED. But in a disaster, it
would quickly transform into a state-of-the-art fa-
cility that could take many times the normal pa-
tient load while providing specialized care and
protection found nowhere else.
Planners hope ER One would not only greatly
enhance the emergency preparedness of the na-
tion’s capital, but also help spur a revolution in
the way the rest of the country and the world
think about modern ED design.
“We have this historical approach to building
hospitals that comes out of the Middle Ages,”
said Craig F. Feied, MD, an emergency physician
and founding director of Project ER One. “This is
not just an emergency room problem — this is a
hospital problem.”
Project leaders have drafted designs and are
ready for an official groundbreaking. Before that
can happen, however, the federal government
has to step in. MedStar Health, the nonprofit hos-
pital network that runs the center, has made an
initial commitment of $25 million to begin con-
struction. The project’s designers are looking for
about another $75 million from the federal gov-
ernment to move into the building phase.
“It is arguably one of the smartest investments
that Congress could make, and it deserves to be
approved,” former Dept. of Health and Human
Services Secretary Tommy Thompson wrote in a
recent editorial in the newspaper The Hill.
But in each of the last two years, ER One fund-
ing has become a casualty of congressional ac-
tion to strip special projects out of budget legisla-
tion. Supporters hope 2007 is the year Congress is
finally convinced of the need for a modernized
emergency department in the capital.
Project leaders have outlined three core con-
cepts: capacity and scalability, specialized capa-
bility and protection.
Washington Hospital Center has a plan to build the nation’s first all-risks-ready
emergency department. But it needs millions in federal funding.
STORY BY DAVID GLENDINNING n ARTWORK COURTESY OF WASHINGTON HOSPITAL CENTER/PROJECT ER ONE
I
magine this: Terrorists attack Washington, D.C., with a combination of
conventional explosives and a biological agent, killing hundreds of people while
injuring and infecting thousands more. Soon emergency departments across the
area are receiving more patients than they can possibly handle. Long lines of
ambulances with no space to offload patients form at hospital entrances. Patients are
stuck in waiting rooms and hallways when all available beds are taken. EDs become
overtaxed and inaccessible.
An early rendering of the ultramodern ED A drop-off concourse and multiple helipads would maximize patient flow in a disaster.
Continued on next page
DESIGNED DISASTERFOR
5
How can we show
what words alone
can’t easily explain?
Protecting patients, saving lives
Advanced protection features would
minimize the chances that a direct
attack would disable ER One.
Specialized medical capabilities, such
as mass decontamination systems that
the facility could activate after a
chemical exposure, would help the
physicians of ER One handle any
major medical emergency.](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-34-320.jpg)
![PAGE 36
NEXT PAGE
For this story about an innovative kidney
exchange, understanding the basics of the
daisy-chain operation was essential. This is
our scorecard of the players. By adding this
graphic presentation, the story was able to
address the personalities and logistics
behind the whirlwind day. Based originally
on a simple diagram presented by the
hospital, this graphic grew to include more
layers of information to describe the people
involved.
n Safe harbors for technology
donations to physicians are
likely off the table as Democrats
shift focus to IT grant money.
DAVID GLENDINNING
AMNEWS STAFF
Washington Capitol Hill’s leading health
information technology legislation for
2006 died a slow death, but lawmakers
are hoping for a reincarnation of sorts
in 2007.
Congress was unable to come to an
agreement on the health IT issue be-
fore adjourning in December, despite
spending about five months trying to
bridge the gap between two signifi-
cantly different Senate and House
bills. The Wired for Health Care Qual-
ity Act passed the Senate in Novem-
ber 2005, and the Health Information
Technology Promotion Act of 2006
passed the House last July.
In the end, disagreements were too
pronounced between House and Sen-
ate leaders over setting safe harbors
for health IT donations to doctors, pro-
viding grants to technology adopters,
and updating diagnostic code sets
used by hospitals and physicians. This
year, lawmakers will go back to the
drawing board and craft new legisla-
tion rather than reintroduce the same
bills that ground to a halt in negotia-
tions between the houses, congres-
sional aides and lobbyists said.
The new Democratic majority in
n Johns Hopkins
surgeons completed
the nation’s first five-way
kidney swap. Here’s how
they linked living donors
with unrelated recipients.
DAMON ADAMS
AMNEWS STAFF
Hours after making history at
Johns Hopkins Hospital, sur-
geon Robert Montgomery,
MD, PhD, retreated to the soli-
tude of his office. He sat most-
ly in darkness at 10 p.m. and
stared at a poster diagram of
the organ donors and recipi-
ents operated on that day.
There was no champagne
celebration. Just quiet reflec-
tion, and the realization that
he and his colleagues had ac-
complished the first five-way
kidney transplant.
“The day had been kind of surreal.
Then later I thought, ‘Wow, look what
we did,’ ” said Dr. Montgomery, who
headed the transplant team. “It was
one of those great moments in one’s
life, and I just felt so privileged to be
part of it.”
In one day, Dr. Montgomery and
his fellow transplant surgeons simul-
taneously removed five kidneys from
living donors, then placed the organs
in five recipients. Start to finish, the
quintuple transplant took 10 hours
and required six operating rooms.
Johns Hopkins had done triple
swaps before, but it broke new med-
ical ground with the five-way ex-
change. Boldly going there took great
skill, precision, cooperation and coor-
dination. The massive undertaking
required the planning and work of
nearly 100 medical professionals, in-
cluding critical care doctors, nephrol-
ogists, operating room nurses, techni-
cians and pharmacists.
“It’s like an orchestra. You have a
www.amednews.com
AMERICAN MEDICAL NEWS
515 NORTH STATE
CHICAGO, IL 60610
★ ★ ★
CLASSIFIED ADVERTISING – PAGE 29
January 1/8, 2007
VOLUME 50 n NUMBER 1American Medical
Baby bias
Managing a practice that is
family-friendly yet equitable
to non-parents can be tough.
But it can be done.
In Business, page 17
Congress adopts
measures to boost HSAs
Government & Medicine, page 7
IHI kicks off new
patient safety initiative
Professional Issues, page 12
Health plans drive
doctors to tiers
Opinion, page 23
Flu vaccine abundant
Health & Science, page 28
The illegal effect
While politicians are
deadlocked on immigration
and insurance issues, doctors
and hospitals are caught
between helping everyone
and staying in business.
In Government & Medicine, page 5
Understanding the
gender divide
Studies suggest ways to
narrow the outcomes gap
between men and women
with heart disease.
In Health & Science, page 26
23 doctors, 6 ORs, 10 hours, 5 lives
The logistics of an innovative kidney exchange
Leslie Persell and Kristine Jantzi, participants in the five-way kidney
transplant, met for the first time a few days after surgery. “When you think
about who do you admire in this, you think about the teamwork, but you admire
the [donors] who were willing to sacrifice,” said surgeon Dorry Segev, MD.
Continued on next page
Continued on page 4
Congress sends health IT back to drawing board
PHOTO BY KEITH WELLER
PREVIOUS PAGE
St. Joseph’s Hospital in Wisconsin is the
topic of this feature. It is past the planning
stages and is up and running as a facility
geared toward patient safety. To explain the
many innovative design details, it is essential
to show, not just tell. (The entire graphic is
not included, due to space limitations).
Photographs and an architectural rendering
work together to highlight the various
improvements. Meanwhile, the story
discusses other, nonvisual, enhancements
and explores the physician side of the story.
Overlap is minimal between graphic and
story, with each being essential to the overall
treatment.
A M E R I C A N M E D I C A L N E W S A M E D N E W S . C O M M A R C H 2 7 , 2 0 0 6
9
Professional IssuesH E A L T H C A R E L I T I G A T I O N n M E D I C A L E D U C A T I O N n E T H I C S n P R O F E S S I O N A L R E G U L A T I O N
State medical groups resist naturopaths’ licensure push [ PAGE 12 ]
“I
T M A Y N O T S E E M L I K E I T , B U T W E ’R E
actually pretty busy today,” said Mike
Murphy, RN, during a recent tour of St.
Joseph’s Hospital in West Bend, Wis.
He’s right. The place doesn’t seem busy.
Compared with other hospitals, the 80-bed,
$55-million facility that opened in August 2005
seems most notable for what it lacks. There’s no
overhead paging system going off. Nurses and
physicians aren’t racing from room to room and
floor to floor. They’re not chatting loudly at a
central station. Rolling carts don’t make a rack-
et on hard tile floors, and there’s no harsh fluo-
rescent lighting to sting the eyes and depress
the spirit. In the rooms, there are no bickering
patient roommates or cramped families.
That St. Joseph’s, 40 miles north of Milwau-
kee, didn’t sound busy was not a matter of
chance but its designers’ intention. Noise reduc-
tion was one of 12 patient-safety principles at
the heart of what seems to be a new concept in
health care construction.
Since the Institute of Medicine’s 1999 report,
“To Err is Human,” estimated medical errors
kill between 44,000 and 98,000 Americans each
year in hospitals, physicians and other health
care leaders have attacked the problem on mul-
tiple fronts, including stepping up investment
in information technology and reporting errors
to encourage system changes. But when it
comes to incorporating patient-safety precepts
into health care infrastructure design, St.
Joseph’s appears to be a pioneer.
St. Joseph’s has sought to achieve safety by
design by incorporating evidence accumulated
by patient-safety experts, a new
breed of health care architects, its
own medical staff and techniques
used in other high-risk fields.
“It was truly visionary,” said Tim
Flaherty, MD, a Neenah, Wis., radiol-
ogist and immediate past chair of the
National Patient Safety Foundation.
“I’m not familiar with another hospi-
tal that did it from the ground up,
where before a shovelful of dirt was
moved, [safety] designs were done.”
SynergyHealth, which owns St.
Joseph’s, in 2002 committed to build
a hospital to replace its 72-year-old fa-
cility, said John G. Reiling, who led
the venture as CEO before leaving in
January. As the process began, Chief
Operating Officer Barbara L.
Knutzen, RN, asked whether the new hospital’s
design could improve patient safety.
“I’ve been involved with building five new
hospitals and hundreds of millions of dollars of
remodeling in my career,” Reiling said. “No-
body had ever asked that question before.”
As Reiling, Knutzen and others at St.
Joseph’s pondered the notion of designing for
safety, a new movement in health care construc-
tion known as evidence-based design was pick-
ing up steam. A 1998 literature search yielded
about 80 articles examining health care design’s
effect on quality, safety and efficiency. Today
there are more than 700 related citations, said
Kirk Hamilton, an associate professor of archi-
tecture at Texas A&M University and co-author
of a 2004 literature review.
The 2004 study concluded that the patient-
safety evidence is strongest for the following
health care design elements, and St. Joseph’s
has implemented all of them:
l Single-bed rooms. Because they are more
open, it’s possible to have different levels of care
throughout a stay with a minimum number of
error-inducing patient moves and handoffs. Sin-
gle-bed rooms cut noise levels, lower hospital-ac-
quired nosocomial infections, improve doctor-
and nurse-patient communication, and make it
easier for families to stay and keep watch.
SAFETY BY DESIGN
Robert Gibson, MD The ICU, emergency department, radiology and surgical units are adjacent,
making it easier to move the most vulnerable patients, Dr. Gibson said. St. Joseph's maximizes
natural light and minimizes noise to create a less stressful, and hopefully safer, environment.
Reducing medication errors Linda Jansen, RN, scans a label using a new electronic medication administration
record and bar coding system that alerts nurses attempting to give the wrong drug at the wrong time.
Drawing on older technology, pneumatic tubes help quickly move materials around the hospital.
Continued on next page
It takes more than competent
and caring physicians, nurses and
medical staff to prevent medical
errors. At St. Joseph’s Hospital
in Wisconsin, patient safety was
built into the design itself.
Story by Kevin B. O’Reilly, Photos by Callie Lipkin
5
How can we show
what words alone
can’t easily explain?](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-36-320.jpg)
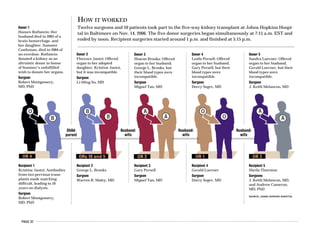

![PAGE 39
What better to accompany a story discussing Medicare’s
payment evolution than the actual mathematical formula
used to figure out pay cuts that doctors may receive. Laying
out in words how cuts are made would be a daunting task, and
a boring read. But this formula is so precise, physicians could
plug in their own numbers. This technical graphic is
particularly good for an audience that is scientifically and
mathematically inclined.
AMERICAN MEDICAL NEWS AMEDNEWS.COM SEPTEMBER 25, 2006
5
CMS chief Dr. McClellan to leave agency [ PAGE 8 ]
MEDICARE / MEDICAID n LEGISLATION AND REGULATION n NATIONAL HEALTH POLICY
Government&Medicine
F
amily physician J. Edward Hill, MD, remembers a time
when physicians who saw Medicare patients were able
to do something that is unheard of today. After the visit,
they would tell the federal government what they thought
was a fair price for their care, and Medicare would pay.
“The reimbursement system was unbelievable,” said Dr.
Hill, American Medical Association immediate past presi-
dent. “You were actually paid what you charged.”
When Dr. Hill started practicing in 1968, near the begin-
ning of Medicare’s life, he charged $3 for a basic office or
home visit. No government-set physician fee schedule
based on rigid mathematical formulas determined this fig-
ure for him.
For nearly 30 years from Medicare’s birth in 1965, the
program operated under some form of the “usual, custom-
ary and reasonable” physician fee system. As long as a doc-
tor quoted his or her usual charge for a procedure and as
long as that figure was within a certain
range of fees that physicians in the same
area were charging for the same service,
Medicare would pay its full share.
The claims process was simple enough
that most doctors did not need the support
staff that they do today to help figure it
out, Dr. Hill said. “My wife was filling out
Medicare claims longhand at the kitchen
table at night and then mailing them the next day.”
Physicians were subject to certain limits in what they
charged, but they would hit these caps only if they raised
fees past the top end of the range. At that point, Medicare
would pay them at the upper limit for that area. If more and
more physicians in the region increased their fees at the
same time, the maximum charge would rise accordingly.
Doctors soon found that they could discover Medicare’s
limits by charging increasingly higher rates until the gov-
ernment checks started coming back short.
Therein lay the major failing of the system, said Stuart
H. Altman, PhD, a health policy professor at Brandeis Uni-
versity in Waltham, Mass. Because federal limits increased
when large numbers of physicians raised their fees, the
amounts that Medicare and many beneficiaries were pay-
ing soon went out of control.
Medicare had adopted this payment structure because it
was demanded by a physician community that was opposed
to the creation of the program in the first place. But much
THE PAYMENT FORMULA
Step 1: Medicare calculates relative value units for each physician service based on how
much a physician is expected to spend on the procedure in terms of work and practice
expenses, including medical liability coverage.
Step 2: The relative value units are adjusted based on the cost of practicing medicine in the
doctor’s geographic area.
Step 3: Medicare calculates the update adjustment factor, of which the sustainable growth
rate is a part. The factor is used to control physician spending in Medicare.
Step 4: The update adjustment factor is multiplied by the Medicare Economic Index,
which is a measure of change in the cost of practicing medicine. The resulting update is a
percentage.
Step 5: The update is applied to Medicare’s conversion factor. This step raises or lowers
physician payment because the conversion factor is then used to turn the relative value
unit totals into dollar amounts. The result is a new payment rate for each physician
service.
crisisto a
Prelude
In 1992 physicians lost the ability to set
their own Medicare prices. The new
payment system seemed to work at first,
but problems quickly ensued.
Next week:
A “rational”
system
unraveled
M E D I C A R E P A Y M E N T
Past Present Futuret
tt
. . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Story by David Glendinning
Illustration by Chris Gash
Continued on next page
................................
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5
How can we show
what words alone
can’t easily explain?
HOW MEDICARE CUTS HAPPEN
Target2006 - Actual2006
Actual2006
X 0.33
Target4/96-12/06 - Actual4/96-12/06
Actual2006 (1 + SGR2007)
UAF2007 = 81.7 - 97.4
97.4
X 0.75 + X 0.33 = -0.280 = -28.0%
693.6 - 741.0
97.4 x 1.007
The physician update adjustment factor (UAF), which helps determine whether physi-
cian fees will go up or down in a given year, is based on a formula set in Medicare
statute. Federal actuaries compare last year’s target physician expenditures, in billions
of dollars, with actual expenditures to see if doctors exceeded the limit. These figures
are modified by the sustainable growth rate (SGR), which is a measure of the econo-
my’s growth, changes in program fees and enrollment, and legislative changes. Here’s
how Medicare will determine the factor for 2007:
UAF2007 = X 0.75 +
SOURCE: CENTERS FOR MEDICARE & MEDICAID SERVICES
But the UAF cannot be more than 3% or less
than -7% in a given year. So for the 2007 calcula-
tion, Medicare uses the lowest possible factor of
-7%. This number is multiplied by the Medicare
Economic Index (MEI), which measures the in-
creased costs to doctors of providing care. The
resulting percentage is applied to Medicare’s
conversion factor, and that’s how the govern-
ment determines next year’s pay:
UAF -7.0%
MEI 2.0%
Calculated 2007
payment change -5.1%
Note: Estimated figures will be finalized Nov. 1.
................................
Using current estimated figures, Medicare can project next year’s adjustment factor:](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-39-320.jpg)
![PAGE 40
Carrying the headline “HHS unveils
local quality reporting plan,” this story
lays out the ambitions of HHS and
addresses the concern physicians have
with yet another quality initiative. The
hypothetical example of a report is an
ideal accompaniment for the top
of the story because it follows the
headline’s prompt: Here’s what’s being
unveiled. Commentary is minimal,
limited to explaining to readers what
they’re viewing.
n The government hopes that local
control will inspire physicians’ trust
and participation. However, some doctors
worry about an overload of competing
quality initiatives.
DAVID GLENDINNING
AMNEWS STAFF
Washington When it comes to publicly reporting the
quality and price of medical services, the Dept. of
Health and Human Services wants to think nation-
ally but act locally.
That’s the driving concept behind the latest HHS
quality and cost initiative, known as “value ex-
changes.” Selected local, nonprofit collaboratives of
health care professionals and purchasers will re-
ceive federal charters to issue report cards for par-
ticipating physicians, nurses, hospitals and others.
By comparing information about multiple care-
givers, health care consumers would be able to de-
cide where to receive treatment based on the quality
of care provided, its price or a combination of both.
A physician who chooses not to participate would
not be listed as an option on the consumer guides.
Although they will follow federal standards in
measuring quality, the collaboratives will be self-
governing. The voluntary effort, part of a broader
n The federal government’s
system for evaluating
requests for marijuana for
clinical study has hindered
investigation of the drug’s
safety and effectiveness, the
opinion states.
AMY LYNN SORREL
AMNEWS STAFF
A decision last month by a Drug En-
forcement Administration judge
could make way for a scientific an-
swer to the controversial question of
whether medical marijuana should be
made available as a prescription drug,
proponents say.
In only the second ruling of its
kind, DEA Administrative Law Judge
Mary Ellen Bittner found that it
would be in the public interest to al-
low a university researcher to grow
cannabis in a licensed facility for use
in privately funded, government-ap-
proved studies to test its potential
clinical benefits.
As a schedule I controlled sub-
stance, cannabis can be researched
only with federal approval. With the
National Institute on Drug Abuse in
control of the supply for U.S. studies,
some doctors and scientists worry
that the government’s tight grip may
be stifling the kind of research used to
test other drugs with therapeutic
possibilities.
In 2005, scientist Lyle E. Craker,
PhD, a professor in the department of
plant and soil sciences at the Univer-
sity of Massachusetts Amherst, ap-
pealed the DEA’s denial of his applica-
tion for a schedule I license to grow
research-grade cannabis for private
AMERICAN MEDICAL NEWS AMEDNEWS.COM MARCH 19, 2007
5
Justice Dept. joins whistle-blower suit about drug pricing fraud [ PAGE 9 ]
MEDICARE / MEDICAID n LEGISLATION AND REGULATION n NATIONAL HEALTH POLICY
Government&Medicine
Percentage of uninsured children
5.6% – 9.9% 10% – 14.9% 15% – 19.9% 20.4%
HHS unveils local quality reporting plan
QUICKVIEW
Kids without coverage
Health reform has returned to center stage this year. With the State
Children’s Health Insurance Program up for congressional reautho-
rization, much of the focus has been on uninsured children. Shown is
the 2003-05 average percentage of children who lack coverage.
SOURCE: GOVERNMENT ACCOUNTABILITY OFFICE ANALYSIS OF CURRENT POPULATION SURVEY
STATISTICS; GEORGETOWN UNIVERSITY HEALTH POLICY INSTITUTE, FEBRUARY
DEA judge’s ruling could help
medical marijuana research
SOURCE: DEPT. OF HEALTH AND HUMAN SERVICES
STATES AND MEDICAL
MARIJUANA
Eleven states have measures
allowing marijuana use for
medical purposes, in spite of
a federal ban:
Alaska Nevada
California Oregon
Colorado Rhode Island
Hawaii Vermont
Maine Washington
Montana
SOURCE: NATIONAL ORGANIZATION FOR THE
REFORM OF MARIJUANA LAWS
Continued on page 8
Continued on next page
5
How can we show
what words alone
can’t easily explain?
SOURCE: DEPT. OF HEALTH AND HUMAN SERVICES](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-40-320.jpg)
![PAGE 41
NOVEMBER 27, 2006 AMEDNEWS.COM AMERICAN MEDICAL NEWS
18
BusinessPRACTICE MANAGEMENT n PERSONAL FINANCE n TECHNOLOGY
Stock option problems magnifying financial troubles for United [ PAGE 22 ]
W
hen one of his two part-
ners left the group, Gene
Murff, MD, an ob-gyn in
Waco, Texas, knew it would im-
pact practice finances. But Dr.
Murff and his remaining part-
ner weren’t sure how much of
an impact to expect.
Fortunately, they had a way
to find out. They use an income
statement to monitor revenue
and expenses for their practice
and use industry statistics to compare it with simi-
lar practices.
“With his leaving it was important to keep an eye
on our expenses to make sure they were consistent
with what the earnings of two physicians would
produce, so it was very helpful,” said Dr. Murff.
Many physicians are discovering just how useful
income statements can be. By spelling out revenue
and expenses, the statements can be used to detect
patterns and reveal how practice finances are
changing. And whether these accounting tools are
prepared with professional help or within the prac-
tice, they can be customized to ensure that physi-
cians get exactly the measurements they need.
With the help of his practice adviser, Dr. Murff
has been using income statements for about 10
years. They have helped him with such things as
staying competitive with staff salaries to revealing
that the practice was spending too much on a type of
injection given to pregnant women.
He believes the effort has paid off in spades. “The
cost in doing this comes back in dividends in what
you learn and savings that you develop.”
Income statements — one of
three major financial state-
ments commonly used by ac-
countants — come in all shapes
and sizes. Generally they in-
clude two major categories:
revenue and expenses, which
are then broken down into
smaller categories and used to
calculate profitability.
Before getting started, ex-
perts say it is important to
determine if accounting will be done on a cash or
accrual basis. Cash-basis accounting notes revenue
and expenses as they are collected or paid, while the
accrual method records revenues and expenses
when they are consummated. Most corporations use
the accrual method. But most physicians find cash-
based accounting gives a better picture of cash flow.
Once the accounting basis is decided, the major
line items can be determined. Revenue can be
broken down into as subcategories, including such
things as third-party payments, co-pay and de-
ductible payments from patients, income from an-
cillary services, interest earned on excess cash, or
proceeds from sales of durable medical equipment.
Regardless if your revenue reflects collections or
charges, accountants stress it is important to record
these figures as accurately as possible. This could
reveal problems in billing and collections, allowing
time to respond before there is major damage.
The second key category of an income statement
is expenses. Again, this can be broken down into
subcategories, including payroll and benefits, drugs
and clinical supplies, office supplies, rent and utili-
Charting your
practice health
Three steps to
making a statement
The three main statements typically
used by financial experts to assess
the health of a practice include the
income statement, balance sheet and
cash flow statement.
Income statement: Identifies rev-
enue, expenses and net profit over a
given period.
Balance sheet: Summarizes financial
health at a given time by listing
assets, liabilities and net worth.
Cash flow statement: Summarizes
cash flow over a given period.
Experts say the income statement
is a good starting point for financial
assessments because it focuses on the
practice’s day-to-day activities.
David E. Hunt, a consultant and
principal with the Waco, Texas-based
accounting firm Parrish, Moody &
Fikes, likened the income statement
to a traffic roundabout. “By looking
at it, you may determine that we need
to go up that highway and see what’s
going on with our clinical supplies, or
we need to go out that highway and
see what’s going on with our payer
mix. This is the first stop. Other
reports may need to be done, but this
is the first stop.” u
— Katherine Vogt
A little extra paperwork can
go a long in way in giving an
accurate picture of your
practice’s financial health.
Story by Katherine Vogt
Illustration by Mario Zucca
The physician world involves lots of
paperwork. This story takes a look at
income statements and the best way for
a doctor to understand his or her prac-
tice’s financial health. While the story
talks to experts about the advantages/
disadvantages of tracking income and
expenses in various ways, it’s the
graphic that gives the exact picture of
what an income statement can be. And
the overlaid text boxes provide an
additional level of usefulness to the
graphic. (Due to space limitations, the
entire graphic is not presented here).
5
How can we show
what words alone
can’t easily explain?
GENERIC MEDICAL PRACTICE — INCOME STATEMENT DEC. 31, 2006
MONTH YEAR
Dec. Dec. 2006 2005
2006 2005
REVENUE
Gross charges Dr. #1 (dollars billed)
Gross charges Dr. #2
Minus adjustments (such as disallowed charges)
Net professional charges
PROFESSIONAL RECEIPTS
Gross receipts Dr. #1 (dollars collected)
Gross receipts Dr. #2
Patient refunds & returned checks
Total professional receipts
GROSS COLLECTION RATIO (gross receipts divided by gross charges)
NET COLLECTION RATIO (gross receipts divided by gross charges, minus adjustments)
GENERAL OVERHEAD EXPENSES
Advertising
Bank charges
Business taxes
Contract fees
Donations
Equipment depreciation and amortization
Equipment lease
Equipment maintenance
Insurance, business
Having month-to-month and
year-to-year comparisons
reveals short-term blips
that need explaining, or
long-term trends that need
to be brought under control.
A collections ratio shows if
you’re getting what you’re
owed. Dividing into gross and
net can show how much you’re
giving to insurers in discounts.
These categories
reflect major expenses,
the items that make up
the practice’s total
overhead. This section
can be detailed or
general, as long as it
gives you the trends
information you need.](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-41-320.jpg)
![PAGE 42
For this feature previewing the year ahead on
Capitol Hill, two key complements were pulled out
in reader-friendly graphics. The first showcased
five lawmakers to watch and outlined some of the
issues they will likely press. The story’s objective
was to explore four medical issues that could make
headlines in the coming year. Meanwhile, the
second graphic adds snapshots of four other issues
that remain of interest to physicians and
lawmakers. The overall package is a smart
handling of the topic, as it balances the emphasis
on the issues as well as the people who have an
impact on the solutions.
OTHER GRAPHIC ON NEXT PAGE
The Texas Republican and
chair of the House Energy and
Commerce Committee helped
shepherd Medicaid reform
through Congress last year.
Expect him to turn his focus
more squarely on the
Medicare payment formula.
The Tennessee
Republican and Senate
majority leader will leave
the upper chamber at
the end of the year.
Expect a big push from
him on medical liability
reform.
A M E R I C A N M E D I C A L N E W S A M E D N E W S . C O M F E B R U A R Y 6 , 2 0 0 6
5
Uncle Sam wants you — for disaster response team [ PAGE 12 ]
M E D I C A R E / M E D I C A I D n L E G I S L A T I O N A N D R E G U L A T I O N n N A T I O N A L H E A L T H P O L I C Y
Government&Medicine
T
HE 2006 LEGISLATIVE SESSION SWINGS
into full gear this month, and lawmakers
once again are prepared to do battle over
health care. In the background, seniors
are trying out new Medicare benefits, and
physicians are readying the fight to accomplish
longstanding legislative priorities.
Although some familiar issues are sure to
make it onto the House and Senate floors, others
appear to be headed toward taking a back seat.
And at least one influential lawmaker on the
health policy scene will say goodbye to Capitol
Hill when 2006 comes to a close.
Here’s a look at what may make headlines
this year.
Medicare’s déjà vu
ONCE AGAIN, PHYSICIANS FACE A MEDICARE
cut that will take effect at the beginning of next
year unless they can procure a rate fix some-
time this session.
The American Medical Association and oth-
er physician groups won’t be content merely to
update reimbursements for a year or to freeze
them at current levels, as Congress decided to
do last year. They are heartened by signs that
lawmakers have heard the call for a more last-
ing solution, said AMA President J. Edward
Hill, MD.
“We’ve done a tremendous job raising aware-
ness of the issue, both on Capitol Hill and with
patients,” he said. “We plan to build on the mo-
mentum from 2005 to make a strong push to re-
place the payment formula with one based on
practice costs in 2006.”
But a minefield of complications could get in
the way of this goal. The already massive price
tag for aligning reimbursements with the cost of
providing care grows with each year of inac-
tion. Medicare spending on such basic physi-
cian services as office visits and imaging proce-
dures also continues to grow at rates that have
drawn the attention of federal officials.
In addition, proponents of permanent physi-
cian payment reform are dealing with a short
time frame to attain their goal. With the
midterm election season starting in earnest in
early fall, any major legislation needs be far
enough along by lawmakers’ August recess to
have a good chance of staying above the fray,
congressional aides said.
Centers for Medicare & Medicaid Services
Administrator Mark McClellan, MD, PhD, sug-
gested in a recent AMNews interview that
physicians might need to make more of a show-
ing in quality reporting programs, the precur-
sor to pay-for-performance, before Congress will
respond with a Medicare payment system over-
haul. Many physicians worry that untested and
misdirected pay-for-performance proposals will
accompany any attempt to pay doctors more
appropriately.
Medicare payment, tort reform
and health IT promise to
keep Congress busy.
Story by David Glendinning
The California Republican and
chair of the House Ways and
Means Committee must step
down from his vaunted chair-
manship at the end of the year
due to term limits. Expect him
to play a big role in physician
pay-for-performance.
The Iowa Republican and chair
of the Senate Finance Commit-
tee has made his reputation
as a tenacious watchdog on
government spending. Expect
him to pay extra attention to
how Medicare is using its drug
benefit dollars.
The Wyoming Republican and
chair of the Senate Health,
Education, Labor and Pensions
Committee had a relatively quiet
2005 at the panel’s helm. Expect
him to make some noise on health
information technology and rural
health care funding.
Sen. Bill Frist, MD Rep. Bill ThomasRep. Joe BartonSen. Charles GrassleySen. Michael Enzi
Lawmakers To Watch
Capitol Hill’s year ahead
P H O T O B Y D E N N I S B R A C K / S T O C K P H O T O . C O M
Continued on next page
6
Can we forecast
or handicap
an issue?
The Texas Republican and
chair of the House Energy and
Commerce Committee helped
shepherd Medicaid reform
through Congress last year.
Expect him to turn his focus
more squarely on the
Medicare payment formula.
The Tennessee
Republican and Senate
majority leader will leave
the upper chamber at
the end of the year.
Expect a big push from
him on medical liability
reform.
The California Republican and
chair of the House Ways and
Means Committee must step
down from his vaunted chair-
manship at the end of the year
due to term limits. Expect him
to play a big role in physician
pay-for-performance.
The Iowa Republican and chair
of the Senate Finance Commit-
tee has made his reputation
as a tenacious watchdog on
government spending. Expect
him to pay extra attention to
how Medicare is using its drug
benefit dollars.
The Wyoming Republican and
chair of the Senate Health,
Education, Labor and Pensions
Committee had a relatively quiet
2005 at the panel’s helm. Expect
him to make some noise on health
information technology and rural
health care funding.
Sen. Bill Frist, MD Rep. Bill ThomasRep. Joe BartonSen. Charles GrassleySen. Michael Enzi
Lawmakers To Watch](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-42-320.jpg)

![PAGE 44
This feature focuses on physician worry that
quality measures could leave behind the sickest
and most vulnerable patients because doctors
don’t want to be dinged on quality measures for
patients they know won’t improve. This box is a
great complement to the story because it answers a
essential question in the debate: Who’s doing the
measuring? The box offers a quick way for readers
to get the names of various groups, who they are
and what they evaluate. It also adds a short URL
for physician readers who want to find out more.
MAY 22/29, 2006 AMEDNEWS.COM AMERICAN MEDICAL NEWS
12
Professional Issues
FSMB data show modest dip in disciplinary actions [ PAGE 15 ]
HEALTH CARE LITIGATION n MEDICAL EDUCATION n ETHICS n PROFESSIONAL REGULATION
C
an a number tell the world how good a doctor is? A lot
of people are counting on it. The government, health
plans and employers are demanding a way to quantify
the value they’re getting for their health care dollars.
Patients, faced with higher co-pays and deductibles and
increasingly invested in health savings accounts, want
reliable public ratings of doctors’ performance.
Only a third of physicians have access to any data about
their own clinical performance, and just a quarter have
the electronic medical records systems considered essen-
tial for continuous quality improvement, according to a
2003 Commonwealth Fund survey of doctors. Still, a small
but growing number of physicians who have assessed the
quality of care they deliver as part of maintenance-of-certi-
fication and pay-for-performance programs see quality
measurement as helpful to care better for their patients.
But many physicians, embittered by early and clumsy
attempts by outsiders to gauge their performance, have
deep concerns about the accuracy and fairness of quality
measurement. With more than 100 pay-for-performance
programs up and running, according to the Leapfrog
Group, and the Centers for Medicare & Medicaid Services
asking physicians to voluntarily report quality data, it
seems quality measurement is here to stay.
Yet as physician groups take over the reins in develop-
ing quality measures for payers and the public to use, a
quandary presents itself: Could attempts to improve quality
by measuring it have the perverse effect of punishing doc-
tors who care for the most vulnerable patient populations?
Skeptical doctors say the medical experts, academicians,
methodologists and statisticians charged with developing
quality measures must be mindful of their potential impact
on practicing physicians and the patients they serve.
Concerns about patient outcomes
R
andall Maxey, MD, PhD, approves of the quality mea-
surement idea in general but worries about whether
its use could wind up penalizing physicians who prac-
tice in underserved areas. While most measures gauge
how often physicians deliver clinically recommended
care, a few very important ones hold doctors accountable
for their patients’ outcomes.
“It’s going to be a lot easier to treat a little old lady from
Beverly Hills,” said Dr. Maxey, an Inglewood, Calif.,
nephrologist who co-chairs the Commission to End Health
Care Disparities and a National Medical Assn. former
president. “Some communities are more compliant and
more health-literate and have more resources to influence
outcomes than others. I may treat you exactly correctly
and give you the right pills, but if you have to choose be-
tween buying pills and giving your baby milk, that drug
may lose out and my performance may be judged as poor
because of it.”
Roy M. Poses, MD, shares Dr. Maxey’s concern.
Qquandary
Quality
PHOTO©JOHNFORASTÉ
ASSESSING
QUALITY
The era of measuring physi-
cian performance is likely
here to stay. Drawn from
a range of perspectives,
experts say these are some of
the pros and cons of quality
measurement.
PROS
n Allows physicians to spot
areas that need improvement
and lets them use the
knowledge to make changes.
n Lets payers reward
physicians who perform
better with more referrals
and bonus pay.
n Empowers consumers to
choose physicians on the
basis of both quality and
cost, particularly with the
number of patients using
health savings accounts at
3.2 million and growing.
Increased competition for
patients will lead to overall
quality improvement.
n Quality measurement can
be inaccurate if it is based on
administrative claims data
that do not capture the
entirety of a patient’s
circumstances.
n Compliance can be costly.
Either a practice must do
timely, expensive chart
reviews or spend heavily on
electronic medical record
systems.
n Quality measures can
unfairly represent
physicians’ performance.
For example, outcome-based
measures can penalize
physicians who see patients
who are sicker or face
economic, cultural and
linguistic barriers to
complying with doctors’
orders.
n When paired with pay-
for-performance, quality
measurement could merely
reward larger practices that
have made costly technology
investments and practices
in higher-income areas.
Perversely, quality measure-
ment could divert resources
away from already under-
served areas.
CONS
As the movement to
measure quality forges
ahead, some physicians
worry their patients
could be left behind.
Story by Kevin B. O’Reilly
Outcome-based measurements need to control for patient characteristics, said internist Roy M. Poses, MD.
7Does the
reader need
the highlights?
WHO’S MEASURING QUALITY?
Several national organizations are involved in setting standards for
how physician quality is, or will be, evaluated. Among them:
THE NATIONAL COMMITTEE
FOR QUALITY ASSURANCE
Who they are: The committee was
founded in 1990 with support
from large employers and the
managed care industry.
What they evaluate: Physician
quality at the health-plan level
via its widely used Health Plan
Employer Data and Informa-
tion Set. Administrative claims
of about 70 million patients, or
85% of all HMO enrollees, are
used to measure physician
performance. The Centers for
Medicare & Medicaid Services
requires HMOs to submit
Medicare HEDIS data.
Web site: http://www.ncqa.org/
PHYSICIAN CONSORTIUM FOR
PERFORMANCE IMPROVEMENT
Who they are: An AMA-convened
group that includes representa-
tives from more than 70 nation-
al and specialty medical soci-
eties, NCQA, CMS, the Agency
for Healthcare Research and
Quality and the Joint Commis-
sion on Accreditation of Health-
care Organizations.
What they evaluate: At press time,
the consortium had developed
93 measures of physician quali-
ty covering 15 conditions, rang-
ing from asthma to osteoarthri-
tis. CMS awarded a contract to
the consortium, NCQA and da-
ta collection firm Mathematica
to develop about 140 measures
covering 34 clinical areas by
year’s end. By December 2007,
the consortium’s measures
should cover the majority
of Medicare spending on
physician services.
Web site: http://www.ama-assn.
org/go/physicianconsortium
NATIONAL QUALITY FORUM
Who they are: Incorporated in
1999, the group doesn’t develop
its own measures, but brings to-
gether consumers, employers,
health plans, researchers,
physicians and others to en-
dorse quality measures.
What they’ve done: NQF so far has
endorsed 36 quality measures
for ambulatory physician care;
24 were developed by the Physi-
cian Consortium for Perfor-
mance Improvement; 12 came
from NCQA.
Web site: http://www.quality
forum.org/](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-44-320.jpg)
![PAGE 45
7Does the
reader need
the highlights?
In this interview, James J. Jordan, of the AMA/State Medical Societies
Litigation Center, discusses what is believed to be the only litigation
center of its kind exclusively for physicians. This graphic is a helpful device
for a reader unfamiliar with the center’s efforts. It highlights four
significant cases that the center has handled. Two of the cases are described
in greater depth during the interview with Jordan, but the graphic’s helpful
labeling allows easy tracking based on issue as well as case name.
AMERICAN MEDICAL NEWS AMEDNEWS.COM JULY 10, 2006
13
Professional IssuesHEALTH CARE LITIGATION n MEDICAL EDUCATION n ETHICS n PROFESSIONAL REGULATION
Insurers using more physician profiling, AMA delegates told [ PAGE 22 ]
I
n an era when physicians appear to be get-
ting as familiar with the courtroom as
they are with the exam room, the Ameri-
can Medical Association/State Medical
Societies Litigation Center is advocating for
doctors by getting involved in the legal system
on their behalf.
Believed to be the only litigation center of its
kind exclusively for doctors, it was established
11 years ago to provide physicians with legal as-
sistance, usually in the form of a friend-of-the-
court brief or a financial contribution. All 50
state medical societies belong, and since its in-
ception in 1995, the Litigation Center has taken
on nearly 150 cases that address issues that have
the potential to make a difference in the prac-
tice of medicine. Peer review, medical liability
reform and physician antitrust issues are just a
few examples of the types of cases the center has
weighed in on.
AMNews reporter Amy Lynn Sorrel recently
talked to Litigation Center Chair James J. Jor-
dan, also executive director of the Alaska State
Medical Assn., about some of the battles perco-
lating in the courts.
AMNews: Are doctors encountering more liti-
gation these days? Why or why not?
Jordan: The answer is yes. And why is that?
There are a lot of confounding and complicating
factors in the life of physicians these days. For
example, the American Academy of Actuaries
did a study back in the late ’90s related to med-
ical liability reform. The [data] indicated that in
the 1950s, physicians had a one in seven chance
of being sued as a result of a medical injury in
their career. By the 1990s, that one in seven
chance was still there, but on a yearly basis.
Also, the relationships between physicians
and managed care organizations and hospitals
are becoming more and more complex. And
the complexity, I hate to say it, often leads to
litigation.
AMNews: What types of cases does the Litiga-
tion Center get involved in?
Jordan: There are three general categories.
The first is what I would refer to as the “David
and Goliath” type cases where an individual
physician or a small group of doctors are, in ef-
fect, overmatched. For example, [we get in-
volved] in disputes involving large managed
care organizations, large hospital systems or
governmental agencies. The second type is a
case usually brought by a state medical society
where the scope of the case may be more direct-
ed towards a specific practice or a geographic
area. However, a lot of times those cases still
AMNews interviews: James J. Jordan
In today’s litigious society, the AMA/State Medical Societies Litigation
Center takes on legal battles in defense of the medical profession.
Interview by Amy Lynn Sorrel n Photographs by Clark James Mishler
Making the case for doctors
Continued on next page
MEDICAID FUNDING
Case: OKAAP v. Fogarty
Major issue: Whether the Oklahoma Medicaid
program violated the “equal access” provision of
the federal Medicaid law because physician pay-
ments were so low that doctors were unwilling
to participate, depriving patients of their rights
to access medical care. The court said yes. The
decision is on appeal, but the state Legislature
has temporarily ordered increased funding to
raise rates.
ERISA
Case name: Kentucky Assn. of Health Plans
v. Miller
Major issue: Whether federal ERISA
requirements regulating health insurance
plans preempt state insurance laws. The U.S.
Supreme Court upheld Kentucky’s “any willing
provider” law, which prevents insurance
companies from discriminating against
doctors who want to join a plan to
provide services.
MEDICAL STAFF
Case: Lawnwood Medical Center v. Lawnwood
Medical Staff
Major issue: Whether a Florida law violated the
contractual nature of medical staff bylaws and ig-
nored a medical staff's right to have a say in hos-
pital governance. The court said yes, and upheld
the bylaws. The hospital said it plans to appeal
the decision, but no formal action has occurred.
ANTITRUST
Case: Higgins v. Baptist St. Anthony’s
Major issue: Whether a Texas hospital and its
health care network violated antitrust laws and
monopolized patient care by keeping physician-
owned hospitals out of the network. The court is-
sued a temporary order saying the network
could not exclude the doctor group until a trial.
The two sides are in settlement talks, and no tri-
al date has been set.
Cases made for doctors
The American Medical Association/State Medical Societies Litigation Center has handled
nearly 150 cases involving a broad range of issues important to physicians. Below are
some highlights. To read more case summaries, visit the Litigation Center’s Web site
(http://www.ama-assn.org/go/litigationcenter).](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-45-320.jpg)
![PAGE 46
7Does the
reader need
the highlights?
This three-part series explored the
past, present and future of Medicare
payments. Illustrations and
typography remained consistent to
lend a cohesive feel for the series,
but the most valuable secondary
component, included with each
installment, is this summary of a
patient visit as it evolves. Its
simplicity is an ideal counterpoint to
the more ambitious stories. As with
each story, it works well on its own,
but when viewed as a complete
package, the trio of graphics provide
an excellent representation of an issue
in transition.
The two other versions of this graphic
are in the Oct. 2 and Oct. 9, 2006, issues. AMERICAN MEDICAL NEWS AMEDNEWS.COM SEPTEMBER 25, 2006
5
CMS chief Dr. McClellan to leave agency [ PAGE 8 ]
MEDICARE / MEDICAID n LEGISLATION AND REGULATION n NATIONAL HEALTH POLICY
Government&Medicine
F
amily physician J. Edward Hill, MD, remembers a time
when physicians who saw Medicare patients were able
to do something that is unheard of today. After the visit,
they would tell the federal government what they thought
was a fair price for their care, and Medicare would pay.
“The reimbursement system was unbelievable,” said Dr.
Hill, American Medical Association immediate past presi-
dent. “You were actually paid what you charged.”
When Dr. Hill started practicing in 1968, near the begin-
ning of Medicare’s life, he charged $3 for a basic office or
home visit. No government-set physician fee schedule
based on rigid mathematical formulas determined this fig-
ure for him.
For nearly 30 years from Medicare’s birth in 1965, the
program operated under some form of the “usual, custom-
ary and reasonable” physician fee system. As long as a doc-
tor quoted his or her usual charge for a procedure and as
long as that figure was within a certain
range of fees that physicians in the same
area were charging for the same service,
Medicare would pay its full share.
The claims process was simple enough
that most doctors did not need the support
staff that they do today to help figure it
out, Dr. Hill said. “My wife was filling out
Medicare claims longhand at the kitchen
table at night and then mailing them the next day.”
Physicians were subject to certain limits in what they
charged, but they would hit these caps only if they raised
fees past the top end of the range. At that point, Medicare
would pay them at the upper limit for that area. If more and
more physicians in the region increased their fees at the
same time, the maximum charge would rise accordingly.
Doctors soon found that they could discover Medicare’s
limits by charging increasingly higher rates until the gov-
ernment checks started coming back short.
Therein lay the major failing of the system, said Stuart
H. Altman, PhD, a health policy professor at Brandeis Uni-
versity in Waltham, Mass. Because federal limits increased
when large numbers of physicians raised their fees, the
amounts that Medicare and many beneficiaries were pay-
ing soon went out of control.
Medicare had adopted this payment structure because it
was demanded by a physician community that was opposed
to the creation of the program in the first place. But much
THE PAYMENT FORMULA
Step 1: Medicare calculates relative value units for each physician service based on how
much a physician is expected to spend on the procedure in terms of work and practice
expenses, including medical liability coverage.
Step 2: The relative value units are adjusted based on the cost of practicing medicine in the
doctor’s geographic area.
Step 3: Medicare calculates the update adjustment factor, of which the sustainable growth
rate is a part. The factor is used to control physician spending in Medicare.
Step 4: The update adjustment factor is multiplied by the Medicare Economic Index,
which is a measure of change in the cost of practicing medicine. The resulting update is a
percentage.
Step 5: The update is applied to Medicare’s conversion factor. This step raises or lowers
physician payment because the conversion factor is then used to turn the relative value
unit totals into dollar amounts. The result is a new payment rate for each physician
service.
crisisto a
Prelude
In 1992 physicians lost the ability to set
their own Medicare prices. The new
payment system seemed to work at first,
but problems quickly ensued.
Next week:
A “rational”
system
unraveled
M E D I C A R E P A Y M E N T
Past Present Futuret
tt
. . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Story by David Glendinning
Illustration by Chris Gash
Continued on next page
................................
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
HYPOTHETICAL PATIENT VISIT
Past Present Futuret . . . . . . . . . . . . . . .
THE SCENARIO: A 68-year-old man whom
the physician has never seen before comes in-
to the office because he now has outpatient
coverage through a new program called
Medicare. Demand for primary care physi-
cians for seniors has skyrocketed since
Medicare’s 1965 inception, and even doctors
who opposed the program’s creation are find-
ing that it has given them a steady stream of
patients.
THE ENCOUNTER: The patient has not seen
a doctor in several years, so the physician
conducts a complete examination and orders
a full range of diagnostic tests. It’s a good
thing that this patient came in, because the
lack of preventive care has contributed to car-
diac and respiratory conditions that require
close monitoring and possible hospitalization
if they worsen.
THE PAYMENT: The physician mails in a
relatively simple paper claims form on which
he has named what he views as a fair price for
all of the covered services. Medicare sends
back a check for the full government share.
Since this patient is relatively well-off, the
physician bills him for the remainder of the
full fee. Although the doctor tries to attract
more of the burgeoning Medicare market by
keeping his charges lower than many nearby
colleagues, he is able to maintain a solid in-
come even after covering all practice costs.](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-46-320.jpg)
![PAGE 47
Name: James J. Jordan
Title: Chair, American Medical
Association/State Medical Societies
Litigation Center; executive director,
Alaska State Medical Assn.
Education: B.A.
Economics, Macalester
College, St. Paul, Minn.
Age: 60
Family: Wife, Karen.
Two Samoyed dogs,
Ice and Zoe.
Hometown: Born in
Walker, Minn. Grew
up in Hibbing, Minn.
Now resides in
Anchorage, Alaska.
Experience: Serves as
executive director of
the Alaska State Med-
ical Assn., a position he
has held for 10 years.
Spent nearly 30 years
in the insurance indus-
try, including time as
director of the Alaska
Division of Insurance.
Retirement aspiration: Remain in Alaska,
but spend time in other, probably warmer,
climates during the darkest winter months.
7Does the
reader need
the highlights?
James J. Jordan was the subject of a feature Q&A and while
he talked about many things, he didn’t mention his dogs, Zoe
and Ice. Sometimes personal details are as interesting as
professional opinions. This feature was part of an ongoing
interview series in Professional Issues that was built around
the idea of presenting prominent people and the issues they
influence. Rather than shift gears mid-interview with
personal questions, this bio box provides a place for such
details. It succeeds by going beyond his alma mater and
bringing more depth to the man. Q&As tend to be an
overused device, as are bio boxes, yet if the profiled person is
worthy of page 1 or a feature, it’s worth giving the reader
more than quotes.
AMERICAN MEDICAL NEWS AMEDNEWS.COM JULY 10, 2006
13
Professional IssuesHEALTH CARE LITIGATION n MEDICAL EDUCATION n ETHICS n PROFESSIONAL REGULATION
Insurers using more physician profiling, AMA delegates told [ PAGE 22 ]
I
n an era when physicians appear to be get-
ting as familiar with the courtroom as
they are with the exam room, the Ameri-
can Medical Association/State Medical
Societies Litigation Center is advocating for
doctors by getting involved in the legal system
on their behalf.
Believed to be the only litigation center of its
kind exclusively for doctors, it was established
11 years ago to provide physicians with legal as-
sistance, usually in the form of a friend-of-the-
court brief or a financial contribution. All 50
state medical societies belong, and since its in-
ception in 1995, the Litigation Center has taken
on nearly 150 cases that address issues that have
the potential to make a difference in the prac-
tice of medicine. Peer review, medical liability
reform and physician antitrust issues are just a
few examples of the types of cases the center has
weighed in on.
AMNews reporter Amy Lynn Sorrel recently
talked to Litigation Center Chair James J. Jor-
dan, also executive director of the Alaska State
Medical Assn., about some of the battles perco-
lating in the courts.
AMNews: Are doctors encountering more liti-
gation these days? Why or why not?
Jordan: The answer is yes. And why is that?
There are a lot of confounding and complicating
factors in the life of physicians these days. For
example, the American Academy of Actuaries
did a study back in the late ’90s related to med-
ical liability reform. The [data] indicated that in
the 1950s, physicians had a one in seven chance
of being sued as a result of a medical injury in
their career. By the 1990s, that one in seven
chance was still there, but on a yearly basis.
Also, the relationships between physicians
and managed care organizations and hospitals
are becoming more and more complex. And
the complexity, I hate to say it, often leads to
litigation.
AMNews: What types of cases does the Litiga-
tion Center get involved in?
Jordan: There are three general categories.
The first is what I would refer to as the “David
and Goliath” type cases where an individual
physician or a small group of doctors are, in ef-
fect, overmatched. For example, [we get in-
volved] in disputes involving large managed
care organizations, large hospital systems or
governmental agencies. The second type is a
case usually brought by a state medical society
where the scope of the case may be more direct-
ed towards a specific practice or a geographic
area. However, a lot of times those cases still
AMNews interviews: James J. Jordan
In today’s litigious society, the AMA/State Medical Societies Litigation
Center takes on legal battles in defense of the medical profession.
Interview by Amy Lynn Sorrel n Photographs by Clark James Mishler
Making the case for doctors
Continued on next page](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-47-320.jpg)
![PAGE 48
Reporter (text file)
Following a conversation with topic editor and
art director to clarify the point of the graphic, the
reporter builds the S1. Working from source data
(not estimates or already plotted graphics) the S1
file should include a suggested head, abstract,
data for graphic and a source line. After checking
work and calculations, the reporter gives a
printout of the data or the link for an online
report to the topic editor and to the art director
working on the assignment. Any calculations
unique to our handling of the data should be
provided as well.
Topic editor first review (text file)
The topic editor double-checks all reporter calcu-
lations and data entry to ensure that the Word file
is accurate; and refines the abstract and suggested
headline. The topic editor provides a printout or
link to the online report to George, who is the
point person on the copydesk for data-intensive
files. Any available calculations also go to George.
In his absence, Pam will delegate the task.
Copydesk/George (text file)
Graphic material, like all text, will continue to
receive two passes through copydesk. In addition,
George will compare the data input in the Word
file against the source data and will check
calculations again.
Art Department (page production)
The art director builds the charts and checks
own work to ensure that errors have not been
introduced in the plotting stage. The art director
works with copydesk/topic editor to adjust any
display language to maximize the graphic’s
clarity on the page and makes sure any changes
in Quark revert to the Word file.
George’s 2nd review (page proof)
In addition to the typical scrutiny given every
page, George will review graphics for errors that
could have been introduced in the plotting
process by comparing the final graphics to source
data. In George’s absence, Pam will delegate the
task.
Topic editor 2nd review (page proof)
Topic editor does final review for potential
errors introduced during plotting. This is also
the last opportunity to review display type and
ensure the graphic is as concise and effective as
originally intended.
The proofing process
This is the new proofing protocol to be
put in place immediately. All tables and
plotted data sets are to follow this process.
Bullet boxes can use the typical [cq] to
signal that quoted numbers and proper
names have been double-checked.
n How to make a quality graphic
n Seven questions to ask
yourself when creating a graphic
n Math concepts every
journalist should know
Graphic
handbook
AMERICAN MEDICAL NEWS](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-48-320.jpg)
![PAGE 49
Definition of percent
Percent means per hundred. Ten percent means
10 per hundred.
If you leave a 10% tip, you’ve given the server a
dime per each $1 of food.
10% = 10 = .10
100
How to calculate a percent
Of 350,000 residents of Buffalo, 300,000 say they
“worship” Nathan Davis. What percent is that?
part x 100% = percent that the part
whole is of the whole
300,000 x 100% = .86 x 100% = 86%
350,000
How to change a percent
into a regular number
Among Lake Shore Athletic Club’s 500 members,
40% work out every day. How many is that?
whole x percent = part
500 x 40% = 500 x 0.40 = 200
How to calculate a percent change
(new value -- old value) x 100% = percent
old value change
There is a difference between a
percent change and a percentage point
A town raises its sales tax rate from 1% to 2%
n The tax rate has increased by one
percentage point.
n The tax one pays on any given pur-
chase has increased 100%, or doubled.
It is a common error for journalists in a case
like this to write that the tax rate increased 1%,
when in fact it rose one percentage point.
In reporting on polls, it is incorrect to say “the
margin of error is 3%.”
n Say: “The margin of error is three
percentage points.”
Do not average percentages
70% of the men in a group like “Grey's Anatomy”/
90% of the women do. Does that mean 80% of
everyone in the group likes “Grey's Anatomy”?
n Answer: Only if the group contains
equal numbers of men and women.
Generally, averaging percentages is a
bad idea.
Math concepts every
journalist should know
Reporters should add a notes mode [cq] to
signal that he/she has double-checked
quoted numbers and proper names.
n How to make a quality graphic
n Seven questions to ask
yourself when creating a graphic
n The proofing process
Graphic
handbook
AMERICAN MEDICAL NEWS](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-49-320.jpg)
![PAGE 50
Math concepts every
journalist should know
Reporters should add a notes mode [cq] to
signal that he/she has double-checked
quoted numbers and proper names.
n How to make a quality graphic
n Seven questions to ask
yourself when creating a graphic
n The proofing process
Never round a number more than once
Round 10.45 to the nearest whole number
Right Wrong
10.45 10.45
10 10.5
11
Understand margins and ratios
A margin has to do with the difference between
two numbers, while ratio deals with proportion.
If the incumbent beats the challenger
200 to 100, then:
n The incumbent beat the challenger by
a margin of 100 votes. (200-100 = 100)
n The incumbent beat the challenger by
a ratio of 2 to 1. (200/100 = 2/1)
There are three types of averages
1. The arithmetic mean: You add all the items
together and divide by the number of items.
2. The median: You list all the items by size. The
median is halfway down the list.
The mean alone can be misleading. If the mean
salary for a practice is $100,000, it would suggest
everyone is highly paid. But if it’s a one-doc
practice and the remaining staff are low-paid
office workers, the mean will be large because one
number is very large. The median and the mean
together give a better idea of the spread of the
numbers. If that one physician earned $175,000
in an office of three employees, then the median
income would be quite low. On the other hand, if
the median is quite near to the mean, it suggests
the income distribution is evenly balanced.
3. The mode: The most frequently occurring item.
Example: In the list of men’s shoe sizes
below, 9 is the mode.
Shoe sizes: 6, 8, 8, 8, 9, 9, 9, 9, 9, 10, 10, 12, 15
Graphic
handbook
AMERICAN MEDICAL NEWS](https://image.slidesharecdn.com/alt-story-formsama-news-1221760910044400-9/85/Alt-Story-Forms-AMA-News-50-320.jpg)

This document provides guidance on creating effective graphics to accompany written articles. It discusses the importance of understanding the data and context before presenting it visually. Key tips include having a clear purpose for the graphic, asking questions to ensure the appropriate comparisons or explanations are shown, vetting the data thoroughly, and collaborating with editors and designers. The document also lists seven important questions graphic creators should ask themselves to determine the best way to visually convey essential information to readers.









































































