

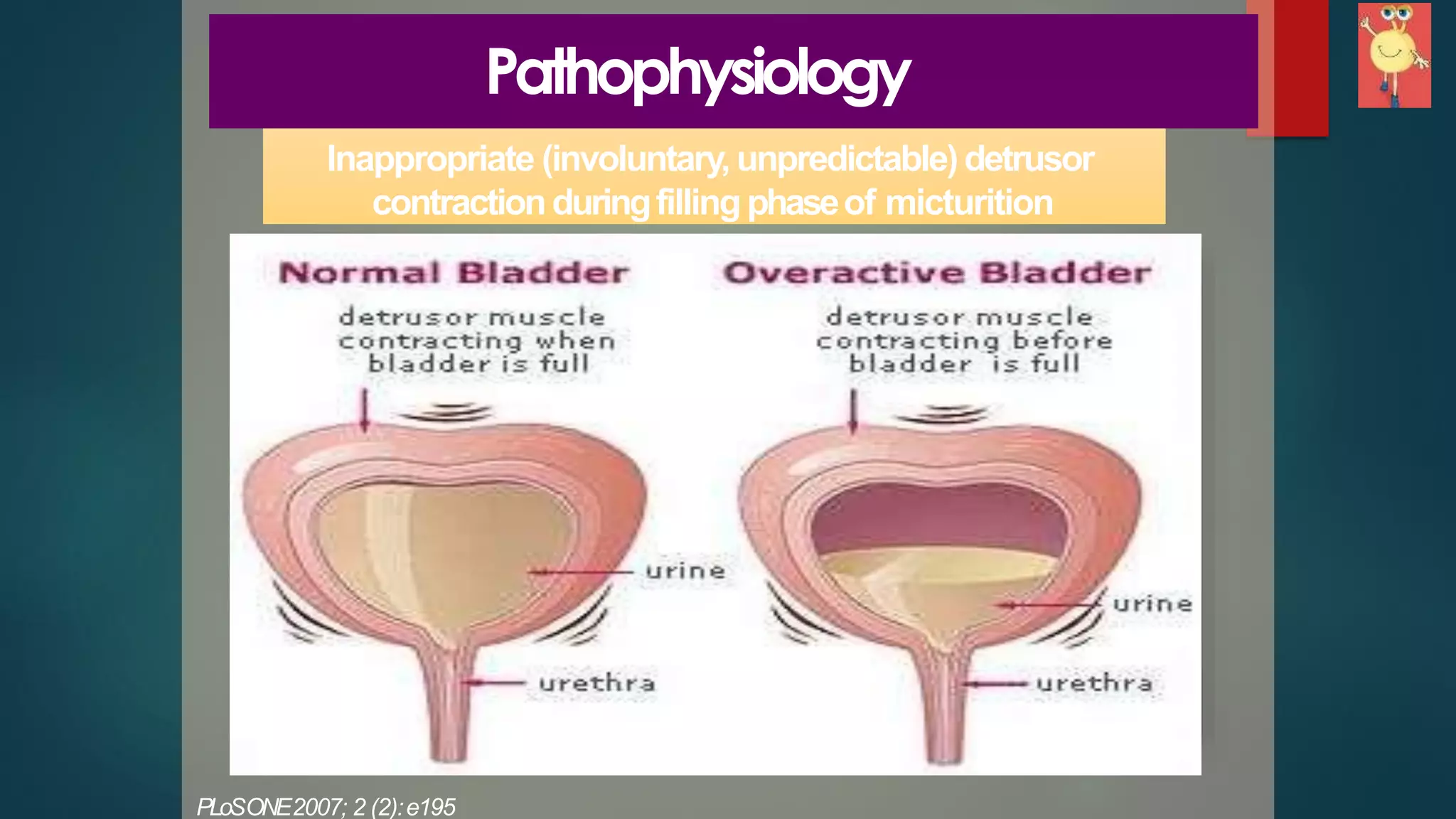








Overactive bladder (OAB) is a prevalent symptom affecting quality of life, particularly in the aging population, characterized by urgency and urge incontinence. Treatment options range from first-line behavioral therapies to pharmacologic management with antimuscarinic agents, which are effective but may have side effects. For refractory cases, third-line treatments include onabotulinum toxin A injections or surgical options such as sacral neuromodulation.













![Interstitial cystitis[1]](https://cdn.slidesharecdn.com/ss_thumbnails/interstitialcystitis1-150315053919-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)




![Incontinence & Female Urology [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/incontinencefemaleedmond-140716213134-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)




































































