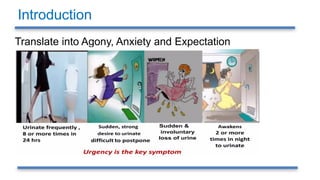
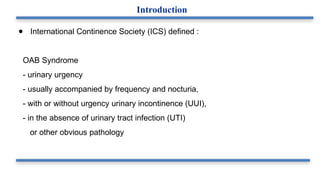
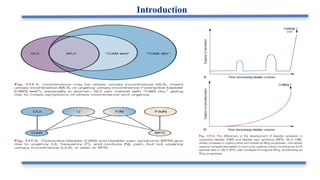
● International ContinenceSociety (ICS) defined :
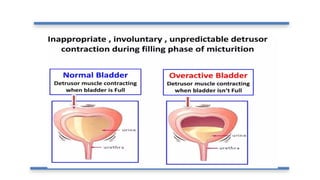
OAB Syndrome
- urinary urgency
- usually accompanied by frequency and nocturia,
- with or without urgency urinary incontinence (UUI),
- in the absence of urinary tract infection (UTI)
or other obvious pathology
Introduction
● OAB withaging
- in women in 40s
- in men in 50s and 60s
● Fewer than 6% report taking medication for their symptoms
● Symptom progression - 1% / year
● Remission - 6% / year
Epidemiology
11.
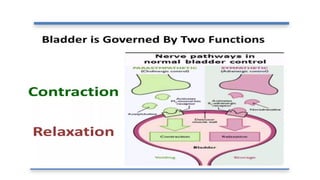
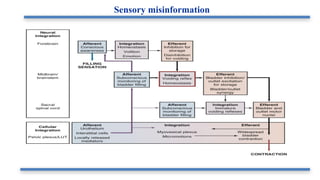
● Multifactorial
● Researchreveals 3 key aspects :
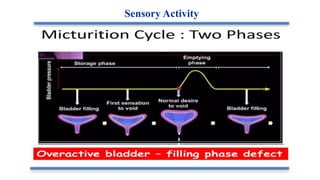
- Sensory activity
- Motor control
- Reflexes of LUT
Pathophysiology and Etiology
● Diagnosis ofOAB is symptom based and involves:
- Careful history
- Physical exam
- Urinalysis
- Frequency volume chart
- Post-micturition residue
Clinical Evaluation
17.
History should coverthe following:
- Presence or absence
- severity, and
- effect on quality of life
for each of the OAB symptoms including
- urgency,
- frequency,
- incontinence.
Other LUTS should also be assessed.
- Presence or absence of dysuria and hematuria.
- Nature and volume of fluid intake.
- Neurologic disease.
Clinical Evaluation
18.
History should coverthe following:
- Obstetric and gynecologic history,
- Previous surgery/ radiotherapy,
- Bowel symptoms.
- Other medical issues (e.g., closed-angle glaucoma, cognitive
impairment can limit treatment options).
- Drug history
- Medications that can exacerbate the symptoms of OAB
(diuretics, alpha agonist)
Clinical Evaluation
19.
Physical examination shouldcover the following:
- Abdominal and vaginal examinations
- Rectal examination should also be undertaken.
- Presence of pelvic organ prolapse, (cystocele may cause urinary urgency and
frequency as it drags on the trigone and causes sensation of bladder fullness.)
- Bimanual examination (r/o pelvic masses,ovarian cysts and uterine
enlargement)
Physical Evaluation
20.
Other possible causesof urgency and frequency of micturition
• Urological:
- Urinary tract infection,
- Bladder tumour,
- Bladder stone,
- Urethral diverticulum,
- Small capacity bladder,
- Interstitial cystitis,
- Radiation cystitis.
● Medical: UMN lesion (Cerebro-vascular stroke , parkinson’s), Impaired
renal function, CCF ,Diabetes mellitus, Diabetes insipidus.
Evaluation
21.
• Urine analysis
-To exclude an underlying UTI.
• Post-micturition residual
• To rule out overflow incontinence or incomplete bladder
emptying, which can cause symptoms of OAB.
Evaluation
22.
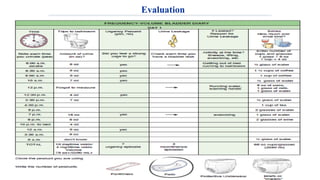
• Bladder diariesare useful tool when assessing patients with urinary
symptoms and facilitates history taking.
• Bladder diary done for a minimum of 3 days and the patient continue his
normal eating/drinking patterns as well as daily activities.
• Record of how much fluid intake , how much urine output , and how often
patient empty his bladder on a daily basis.
Evaluation
Patient Perception ofIntensity of Urgency Scale (PPIUS) is a five-point scale designed to rate
the level of urinary urgency
1. No urgency: felt no need to empty my bladder but did so for other reasons.
2. Mild urgency: could postpone voiding for as long as necessary without fear of
wetting myself.
3. Moderate urgency: could postpone voiding for a short while without fear of wetting
myself.
4. Severe urgency: could not postpone voiding but had to rush to the toilet to avoid
wetting myself.
5. Urgency incontinence: leaked before arriving at the toilet.
Evaluation
25.
● Urodynamic indicatedwhen
- Conservative and drug therapy fail adequately to manage OAB.
- Complicated cases of OAB.
- Before invasive surgery.
● Whether to discontinue anti-muscarinic drugs before the test can be argued
either way;
- Stopping the drugs (48 hr.) gives the best chance of observing DO if present.
• Two main urodynamic finding associated with OAB are DO and increased filling
sensation.
Evaluation
• Non invasiveTreatment :
- Behavioral therapy
- Oral Medication ( anticholinergic or beta 3 agonist)
- Combined therapy:behavioral and pharmacologic therapy.
- Estrogen for postmenopausal women.
- Role of alpha blocker.
• Minimally invasive Treatments:
- Botulinum A-toxin.
- Neuromodulation (post tibial nerve , sacral nerve stimulation)
- Interruption of innervation (central subarachnoid block or sacral rhizotomy,
Peripheral motor and/or sensory block)
• Highly invasive Treatments: Augmentation cystoplasty, Urinary diversion.
Treatment
28.
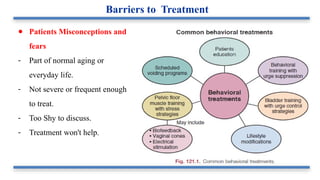
● Patients Misconceptionsand
fears
- Part of normal aging or
everyday life.
- Not severe or frequent enough
to treat.
- Too Shy to discuss.
- Treatment won't help.
Barriers to Treatment
29.
● Dietary Changesand fluid Management
- Weight loss in obese patient.
- Cessation of smoking.
- Avoid Diuretics and excessive fluid intake especial
before bed time.
- Treat constipation.
• Foods and drinks should avoided in overactive bladder
(bladder irritants).
- Spicy foods
- Coffee
- Alcohol
- Soda
- Orange juice
- Tomatoes (acidic)
- Chinese Flavor (Monosodium Glutamate )
Behavioral Modifications
30.
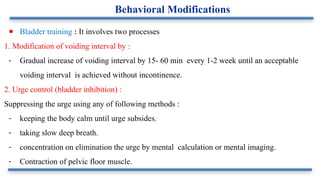
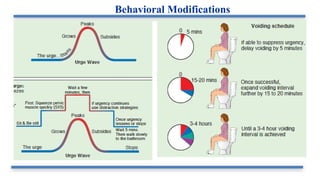
● Bladder training: It involves two processes
1. Modification of voiding interval by :
- Gradual increase of voiding interval by 15- 60 min every 1-2 week until an acceptable
voiding interval is achieved without incontinence.
2. Urge control (bladder inhibition) :
Suppressing the urge using any of following methods :
- keeping the body calm until urge subsides.
- taking slow deep breath.
- concentration on elimination the urge by mental calculation or mental imaging.
- Contraction of pelvic floor muscle.
Behavioral Modifications
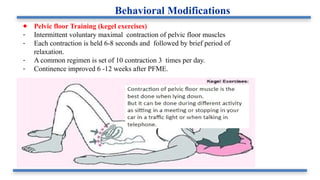
● Pelvic floorTraining (kegel exercises)
- Intermittent voluntary maximal contraction of pelvic floor muscles
- Each contraction is held 6-8 seconds and followed by brief period of
relaxation.
- A common regimen is set of 10 contraction 3 times per day.
- Continence improved 6 -12 weeks after PFME.
Behavioral Modifications
33.
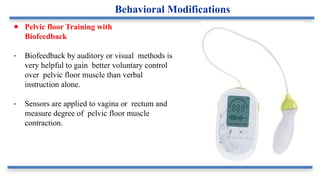
● Pelvic floorTraining with
Biofeedback
- Biofeedback by auditory or visual methods is
very helpful to gain better voluntary control
over pelvic floor muscle than verbal
instruction alone.
- Sensors are applied to vagina or rectum and
measure degree of pelvic floor muscle
contraction.
Behavioral Modifications
● Contraindications :
-Urinary retention
- Intestinal obstruction
- Uncontrolled narrow angle glaucoma
- Myasthenia gravis
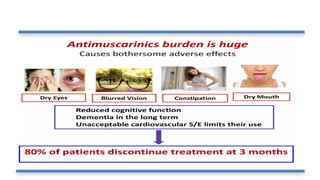
● Duration of treatment :
- It improve symptoms within 1 week but max benefit is achieved by 3
months.
- Over 5o% of patients stop it within 3 months due to
Ineffectiveness, side effect, or cost.
Medication
38.
● Avoid applicationto same skin site with in 7 days.
(abdomen,hip ,buttock)
● 3.9 mg patch, twice weekly (every 3- 4 days)
● It bypasses first-pass hepatic metabolism
● Less active metabolic (N -Desethyloxybutynin)
● So less side effects
- Erythema/pruitis
- Less dry mouth.
● Now, a New : 1g topical gel is also available in US.
● It delivers approx 4g of drug.
Oxybutinin Transdermal patch
Translucent matrix-type patch Twice weekly application
39.
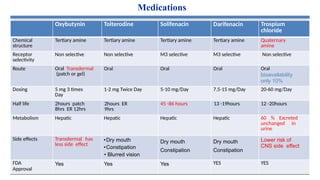
Medications
Oxybutynin Tolterodine SolifenacinDarifenacin Trospium
chloride
Chemical
structure
Tertiary amine Tertiary amine Tertiary amine Tertiary amine Quaternary
amine
Receptor
selectivity
Non selective Non selective M3 selective M3 selective Non selective
Route Oral Transdermal
(patch or gel)
Oral Oral Oral Oral
bioavailability
only 10%
Dosing 5 mg 3 times
Day
1-2 mg Twice Day 5-10 mg/Day 7.5-15 mg/Day 20-60 mg/Day
Half life 2hours patch
8hrs ER 12hrs
2hours ER
9hrs
45 -86 hours 13 -19hours 12 -20hours
Metabolism Hepatic Hepatic Hepatic Hepatic 60 % Excreted
unchanged in
urine
Side effects Transdermal has
less side effect
•Dry mouth
•Constipation
• Blurred vision
Dry mouth
Constipation
Dry mouth
Constipation
Lower risk of
CNS side effect
FDA
Approval
Yes Yes Yes YES YES
● Botulinum A-toxinIntravesical injection.
- Inhibit detrusor contraction by inhibit release
of Ach at neuromuscular Junction.
- FDA approved in treatment of OAB refractory to
Antimuscarinic medications
● Side effects
- Increase risk of UTI and Urinary retention
that required catheterization.
● Contraindications
- UTI, Pregnancy , myasthenia gravis.
Minimally invasive treatment