Downloaded 10 times





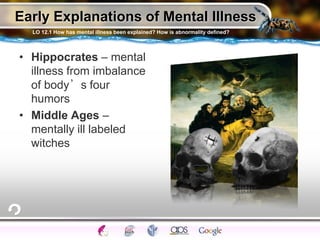














![DSM-IV-TR Psychological Profile Overview
Are Psychosocial or Environmental Problems (school or housing
issues) also present?Axis IV
What is the Global Assessment of the person’s functioning?
(0-100 Point Scale)Axis V
Is a General Medical Condition (diabetes, hypertension or
arthritis etc) also present?Axis III
Is a Personality Disorder or Mental Retardation present?
Axis II
Is a Clinical Syndrome (cognitive, anxiety, mood disorders [16
syndromes]) present?Axis I
22](https://image.slidesharecdn.com/aguiarapabnormal-140310121334-phpapp02/85/Aguiar-ap-abnormal-22-320.jpg)











































































1. Anxiety disorders involve excessive and persistent worries or fears that interfere with daily functioning, unlike ordinary worries or fears. 2. Common anxiety disorders include generalized anxiety disorder, panic disorder, phobias, obsessive-compulsive disorder, and post-traumatic stress disorder. 3. Proposed causes of anxiety disorders include biological factors like abnormal neurotransmitter levels or brain structures, as well as psychological factors like repressed urges, conditioning, or traumatic experiences.































































