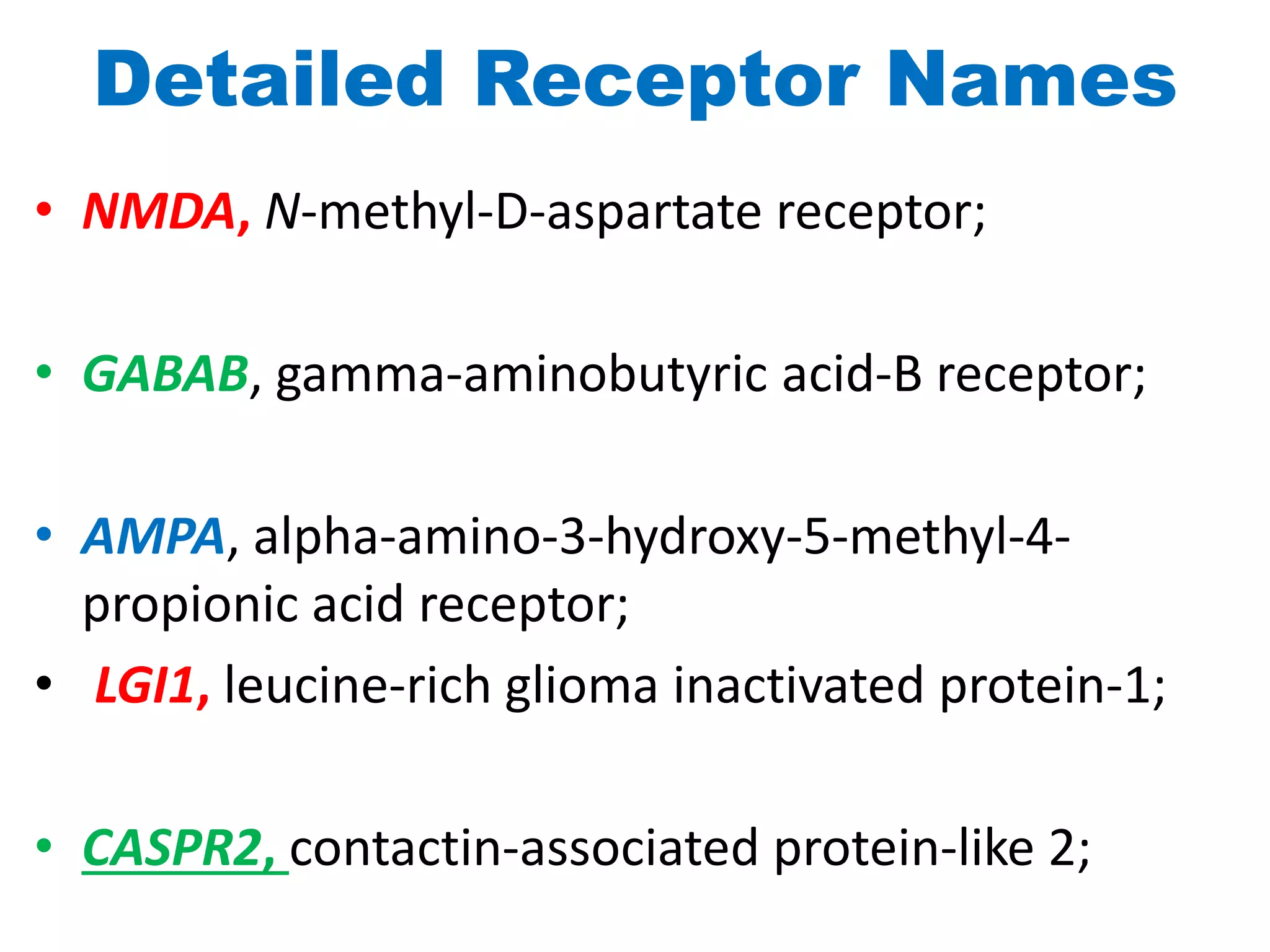
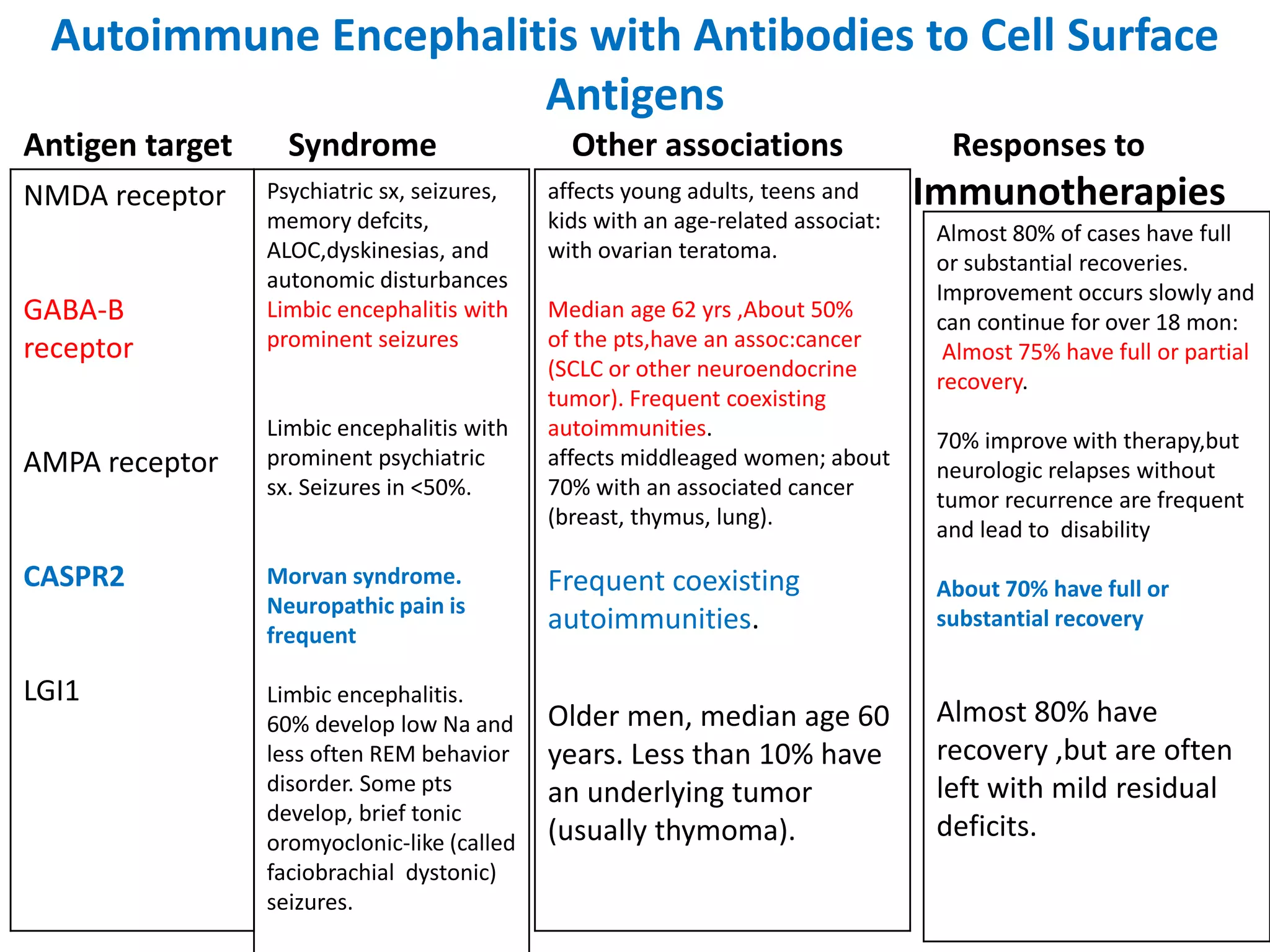
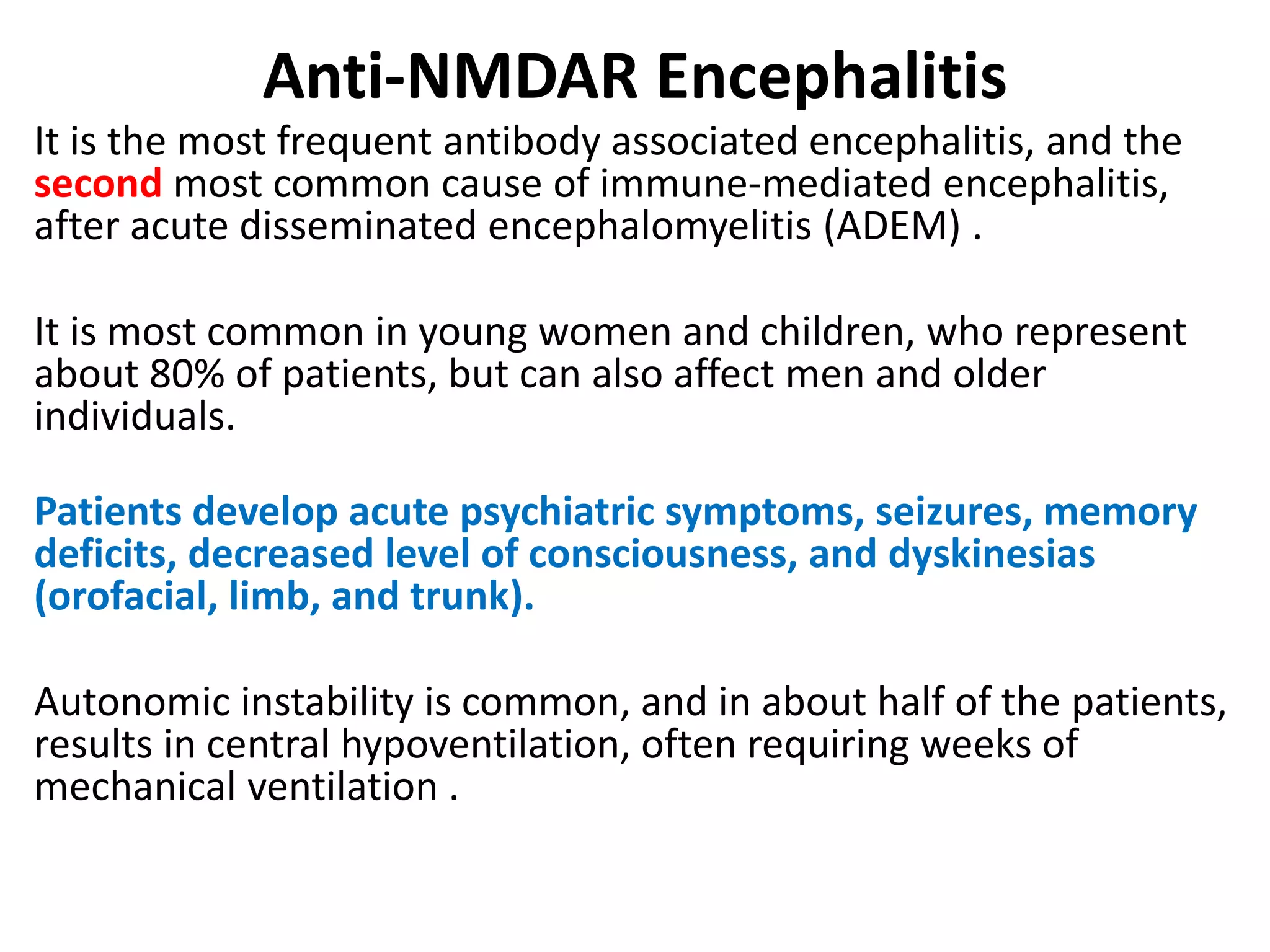
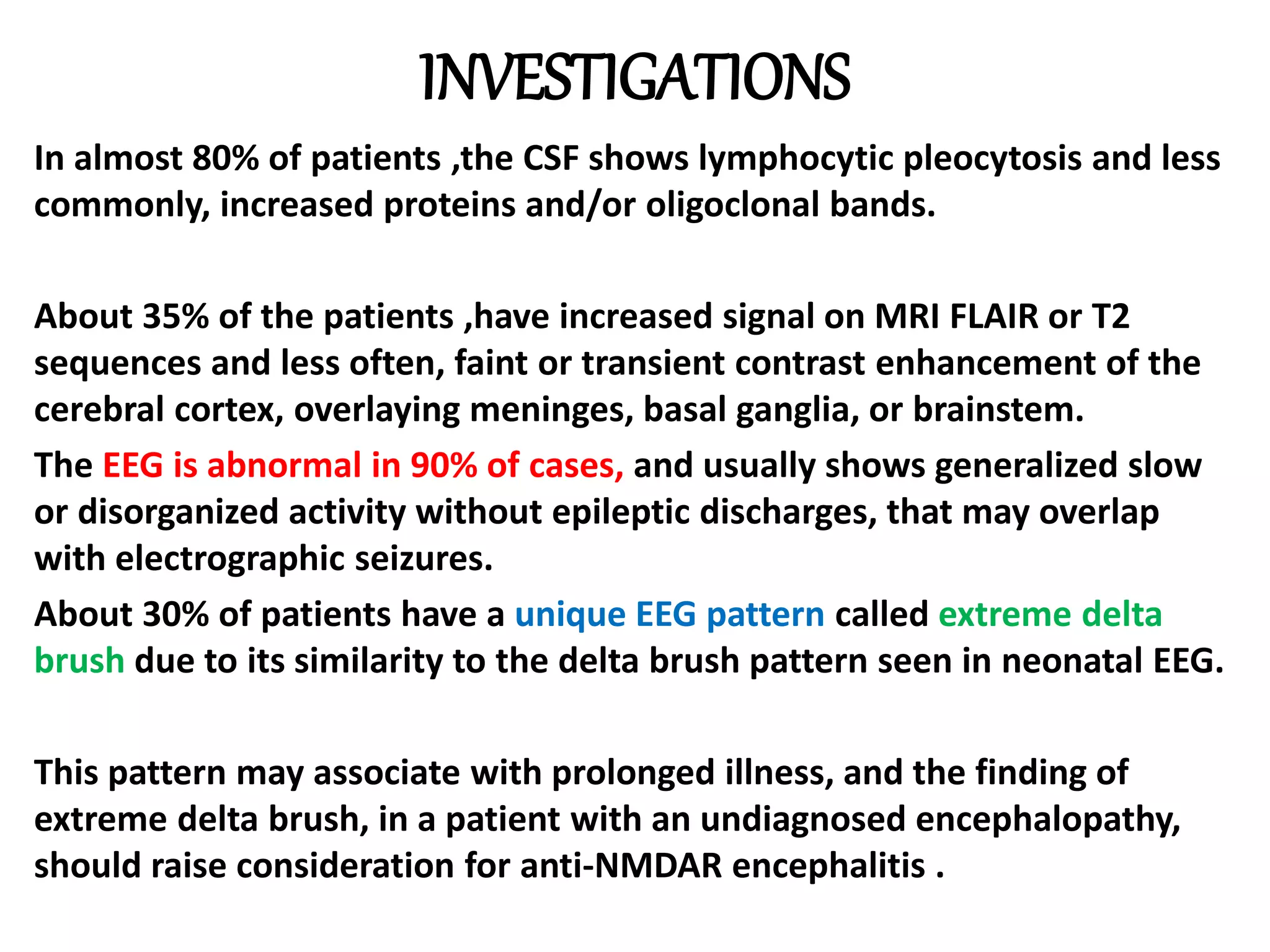
This document discusses autoimmune encephalitis, which is caused by antibodies targeting neuronal cell surface or synaptic antigens. It can present with various neuropsychiatric symptoms and be misdiagnosed as viral encephalitis. Diagnosis is confirmed by detecting antibodies in CSF and serum, often against NMDA receptors. Treatment involves immunotherapy like steroids, IVIg, or plasma exchange. Outcomes are generally good if treated promptly, though some disorders relapse. Tumor removal may also be needed if one is present.














































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)











