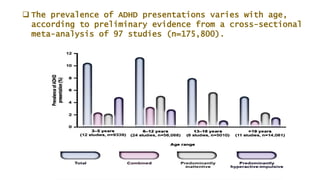
This document provides an overview of attention deficit hyperactivity disorder (ADHD). It begins with an introduction that describes ADHD as a common neurodevelopmental disorder characterized by inattention, hyperactivity, and impulsivity. It then discusses the types of ADHD (predominantly inattentive, predominantly hyperactive-impulsive, and combined type), prevalence rates, etiology, comorbidities, signs and symptoms, diagnosis, prognosis, and treatment options. Treatment involves medication, therapy like cognitive behavioral therapy, behavior therapy, and lifestyle modifications to help manage symptoms.



![In India, a study entitled Prevalence of Attention Deficit Hyperactivity Disorder in Primary
School Children that was conducted in Coimbatore found ADHD prevalence in children to
be higher than the global estimate, at 11.32%. The highest prevalence is found in ages 9
(at 26.4%) and 10 (at 25%). 7.4% globally affected
The study showed that more males (66.7%) were found to have ADHD than females .
The estimated prevalence of ADHD in school-aged children increased from 6% in 1997 to
9% in 2006
[ National Center for Health Statistics, 2006]
9.4% of children and 4% of adult in America are likely to have ADHD [Kessler et al. 2006].](https://image.slidesharecdn.com/adhdpresen-230423074900-74d47557/85/ADHD-PRESEN-pptx-5-320.jpg)
![ Family Studies have shown that 25% closer relatives in the families of ADHD children
have ADHD compared to 5% of general populations.
1/3 of ADHD children have at least one parent who has ADHD.
Twin studies have shown that there is up to 75% increased concordance in
monozygotic twins to develop ADHD as compared to dizygotic twins .
DA Transporter Gene [DAT1]
Dopamine receptor [DRD4, “ Repeater Gene”] is over represented in ADHD patients
Some genetic syndromes like Fragile-X Syndrome , Tuberous Sclerosis etc , can cause
ADHD.](https://image.slidesharecdn.com/adhdpresen-230423074900-74d47557/85/ADHD-PRESEN-pptx-8-320.jpg)
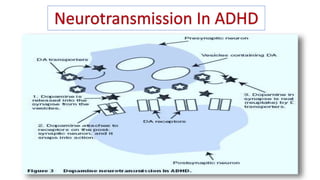
![ There are two main neurotransmitters involved in ADHD:
1] Dopamine and 2]Norepinephrine 3]Serotonine
These neurochemicals have been shown to be involved in impulsive control,
prioritization, focus, decision-making, frustration tolerance, and time management,
among many other important mental processes. The brains of people diagnosed
with ADHD show a deficit in these two key neurotransmitters
Dopamine (DA) is a neurochemical that is considered to be directly linked with our
perception of pleasure and reward. People with ADHD have been observed to have
more dopamine transporters in the brain, which cause less dopamine to be
available.
Norepinephrine (NE) is another neurochemical that is related to dopamine and is
found in lower-than-normal levels in ADHD brains Norepinephrine is involved in
focus, processing, and controlling impulsive behaviors](https://image.slidesharecdn.com/adhdpresen-230423074900-74d47557/85/ADHD-PRESEN-pptx-9-320.jpg)
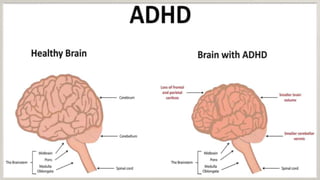
![ The ADHD brain has impaired activity in four functional
regions of the brain.
1] Frontal cortex,
2]Basal ganglia ,3] Limbic system , 4] Reticular activating
system
Reduction in volume and activity of caudate nucleus,
prefrontal cortex white matter , corpus callosum and
cerebellar vermis
Reduction in Globus pallidus and ventral striatum.
Reduction in temporal and superior cortices](https://image.slidesharecdn.com/adhdpresen-230423074900-74d47557/85/ADHD-PRESEN-pptx-11-320.jpg)


![OPPOSITIONAL
DEFIANT
DISORDER
[21% to 60% ]
TOURETT’S
SYNDROME
[55%]
ANXIETY
[Approximately
25% ]
LEARNING
DISORDER
[9% vs 4%,]
CONDUCT
DISORDER
[25% to 40% ]
DEPRESSION
[0 to 30%]
Comorbid conditions are distinct
diagnoses that exist simultaneously with
ADHD.
In general, individuals affected by ADHD
often have other behaviour disorders that
impact their ability to function
successfully.
The comorbidity of ADHD with other
disorders
is between 60% and 80%.
When comorbid conditions are present, it
can make the diagnosis of ADHD much
more difficult to pinpoint and the
symptoms harder to treat.
Some comorbid disorders that commonly
occur alongside ADHD are:
ADHD](https://image.slidesharecdn.com/adhdpresen-230423074900-74d47557/85/ADHD-PRESEN-pptx-15-320.jpg)
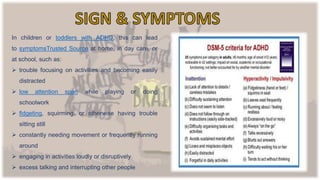



![ADHD-a condition that can cause trouble with focus , patient
and over- activity . Most common childhood disorder.
Three types of ADHD – Inattention , Hyperactive-Impulsive
Combined.
Boys are more likely to have ADHD than girls.
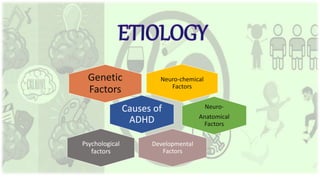
So many causes can result ADHD like genetic factors
neurotransmitters
[ dopamine and norepinephrine] , some environmental
psychological , anatomical Factors.
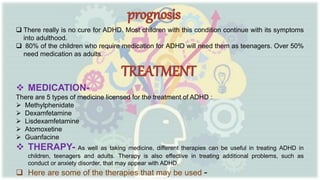
ADHD can’t be cured , but can be managed . In most cases
ADHD is best treated with a combination on medication an
behaviour therapy .
Parents has very important role in treating child with ADHD
They need to build a positive relationship with more efforts tha
general population. They need to understand their child .](https://image.slidesharecdn.com/adhdpresen-230423074900-74d47557/85/ADHD-PRESEN-pptx-22-320.jpg)
![www.verywellmind.com
Kaplan and Saddock’s [Book of Psychiatry]
www.webmd.com
www.healthline.com.
Niraj Ahuja [A Short Book O F Psychiatry]](https://image.slidesharecdn.com/adhdpresen-230423074900-74d47557/85/ADHD-PRESEN-pptx-23-320.jpg)




































































