Downloaded 26 times















![Source: Centers for Disease Control and Prevention. Prevalence of diagnosis and medication treatment for
attention-deficit/hyperactivity disorder – United States, 2003. MMWR 2005;54:[842-847].
86](https://image.slidesharecdn.com/adhdnowell-120503070133-phpapp01/85/Adhd-nowell-84-320.jpg)
![Percent of Youth 4-17 ever diagnosed with Attention-Deficit/Hyperactivity Disorder:
National Survey of Children’s Health, 2003
> 10.1%
9.1 – 10.0%
DC
8.1 - 9.0%
7.1 - 8.0%
6.1 - 7.0%
< 6.0%
Source: Centers for Disease Control and Prevention. Prevalence of diagnosis and medication treatment for
attention-deficit/hyperactivity disorder – United States, 2003. MMWR 2005;54:[842-847].
87](https://image.slidesharecdn.com/adhdnowell-120503070133-phpapp01/85/Adhd-nowell-85-320.jpg)



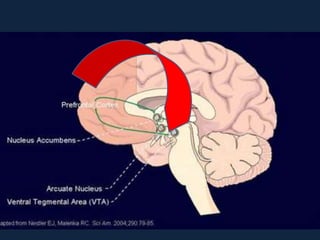






























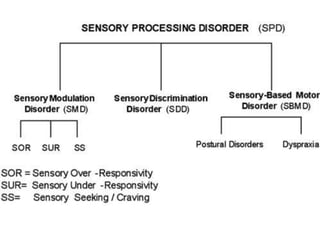
This document discusses ADHD and processing disorders. It begins with an overview of making sense of disorders like sensory processing disorder, central auditory processing disorder, and ADHD with executive dysfunction. It then discusses treatment approaches for these disorders from both "top-down" and "bottom-up" perspectives. The document provides information on diagnostic assessments and controversies around conditions like ADHD.













![Adhd 30 Nov 08 (1)[1]](https://cdn.slidesharecdn.com/ss_thumbnails/adhd-30-nov-08-11-1229375188411368-1-thumbnail.jpg?width=640&height=640&fit=bounds)





































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













