Downloaded 10 times



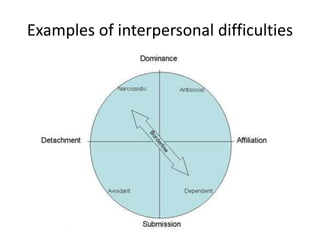







The document discusses the complexities of personality disorders in disability reviews, outlining the domains of dysfunction such as distorted thinking, problematic emotions, impulse control, and interpersonal difficulties. It reviews the causes, treatment options, and diagnostic criteria both under traditional frameworks and the alternative DSM-5 model. Key considerations for documentation and regulatory compliance are highlighted to ensure proper assessment and support in the review process.


















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



