Downloaded 61 times



























![Dr. Daniel Boone La Hacienda Treatment Center 800-749-6160 [email_address]](https://image.slidesharecdn.com/addictionsandthebrain-110916123457-phpapp01/85/Addictions-and-the-Brain-51-320.jpg)

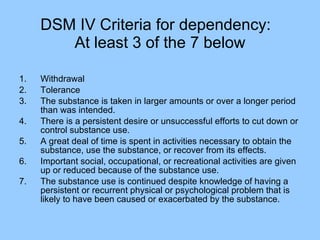
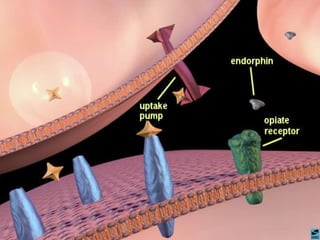
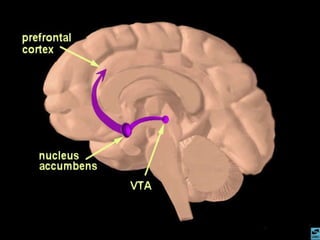
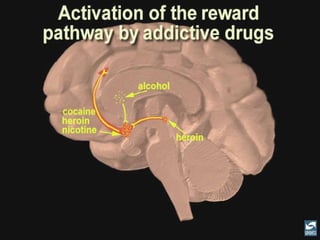
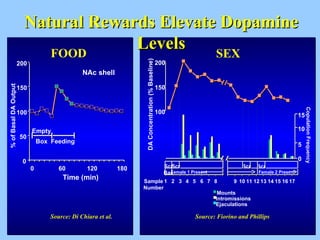
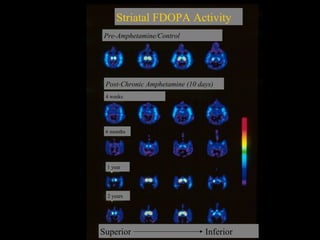
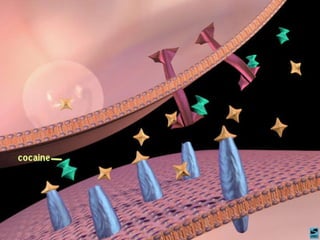
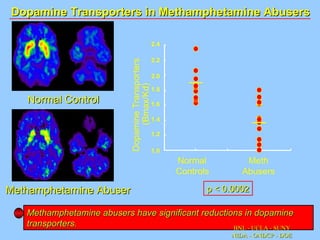
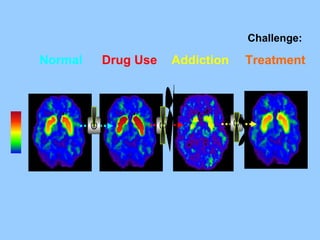
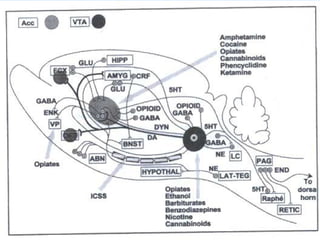
The document discusses addiction as a chronic disease characterized by denial, loss of control, and relapse, outlining diagnostic criteria from DSM IV. It highlights the impact of various substances on dopamine levels in the brain, particularly in methamphetamine abusers, and provides information on relapse pathways and prevention strategies. Additionally, it reviews different medications for addiction treatment, including their mechanisms of action, dosing, and side effects.


















































































