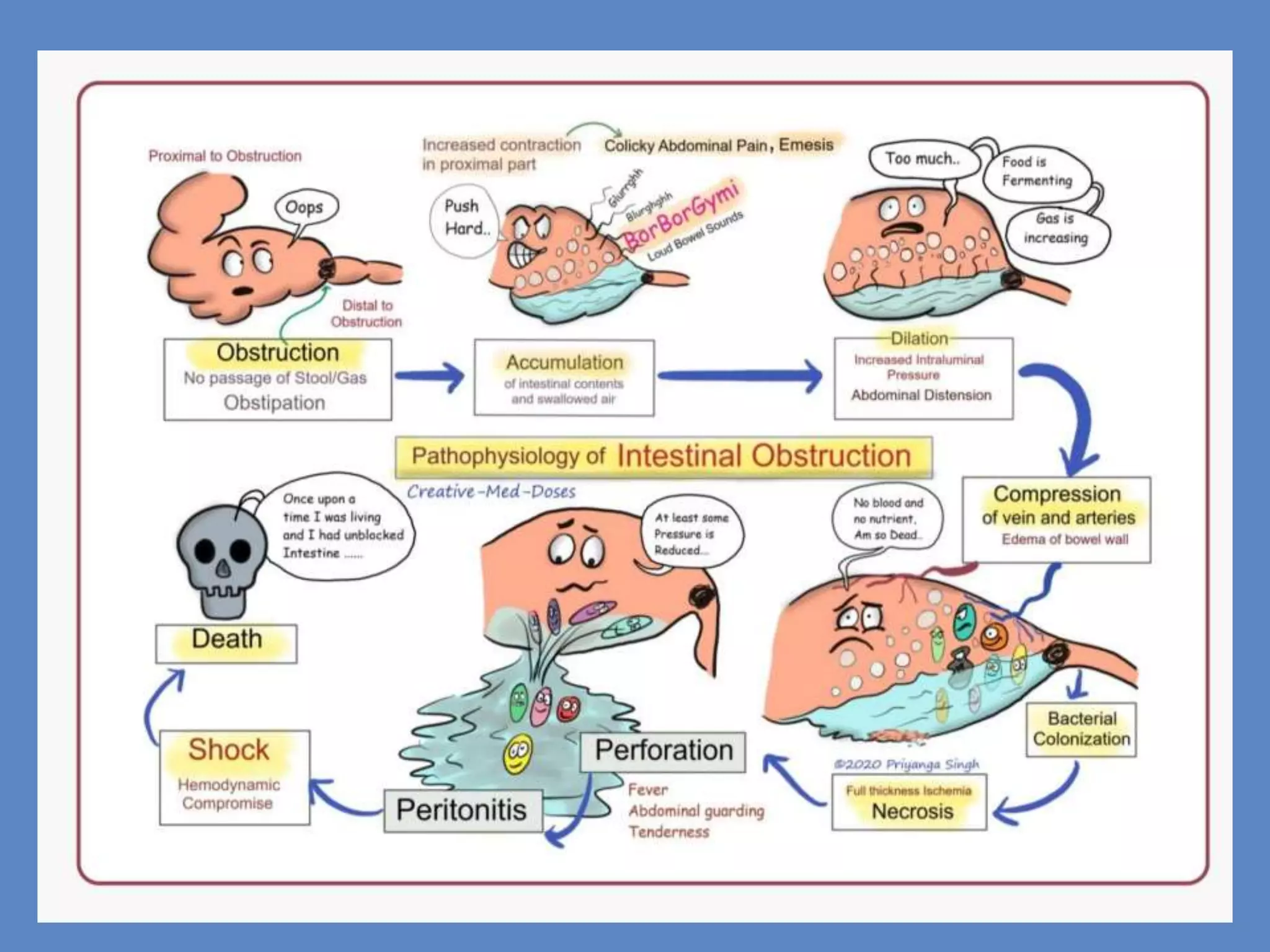
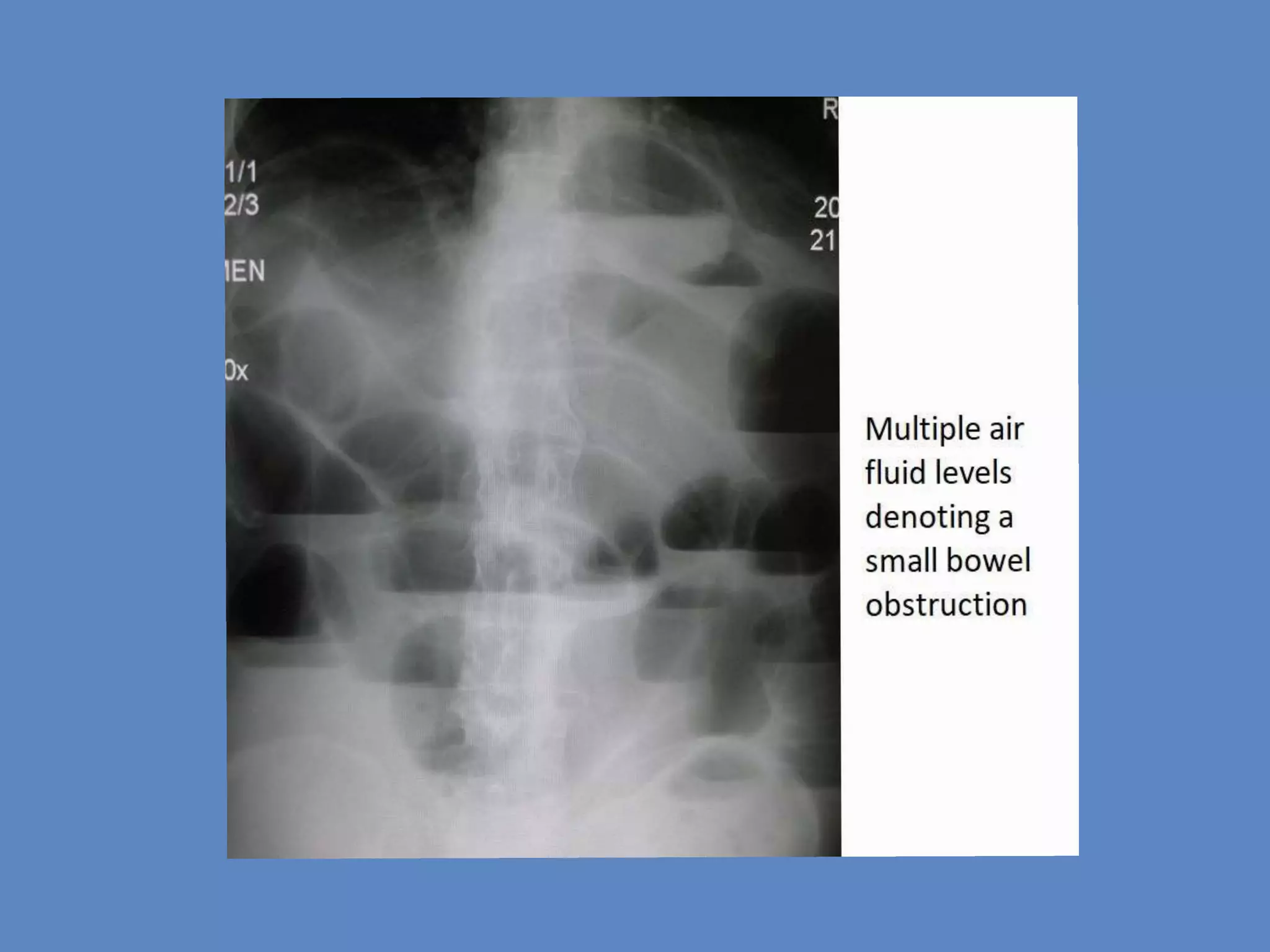
Acute strangulated intestinal obstruction is a severe condition where the blood supply to the intestines is compromised, potentially leading to gangrene and peritonitis. It is characterized by symptoms such as abdominal distention, pain, vomiting, and fever, often requiring surgical intervention for treatment. Risk factors include prior abdominal surgery and conditions like Crohn's disease and cancer.