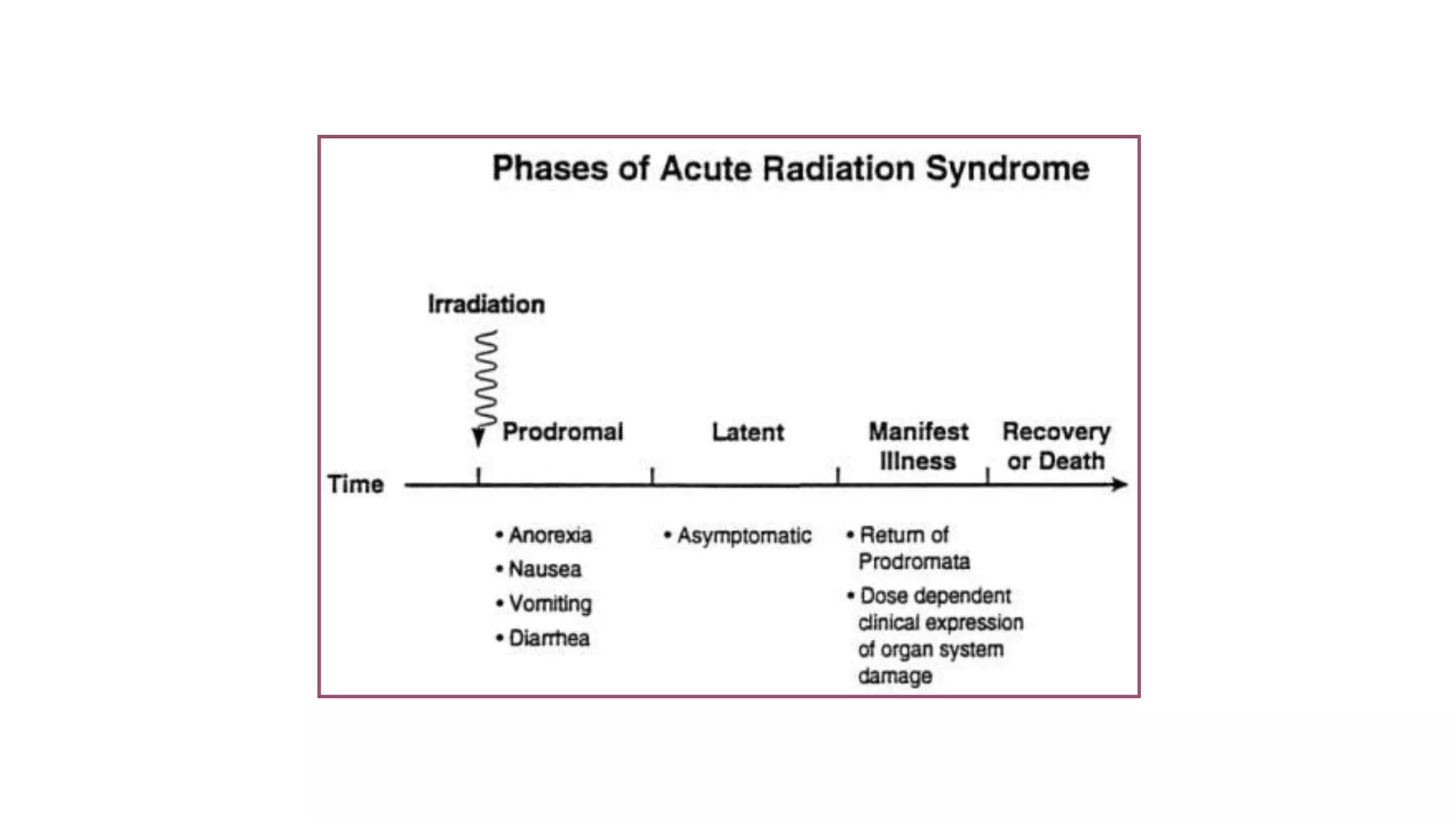
Acute radiation syndrome is caused by exposure to high doses of radiation over a short period of time. There are three main syndromes that develop based on the absorbed radiation dose: hematopoietic syndrome from 1-10 Gy affecting bone marrow, gastrointestinal syndrome from 10-50 Gy, and central nervous syndrome above 50 Gy. Symptoms develop in the prodromal phase within hours, followed by a latent phase with no symptoms for weeks. The critical phase sees a relapse of severe symptoms that can cause death within days depending on the radiation dose. Outcomes depend on factors like radiation type, dose, and rate of exposure.