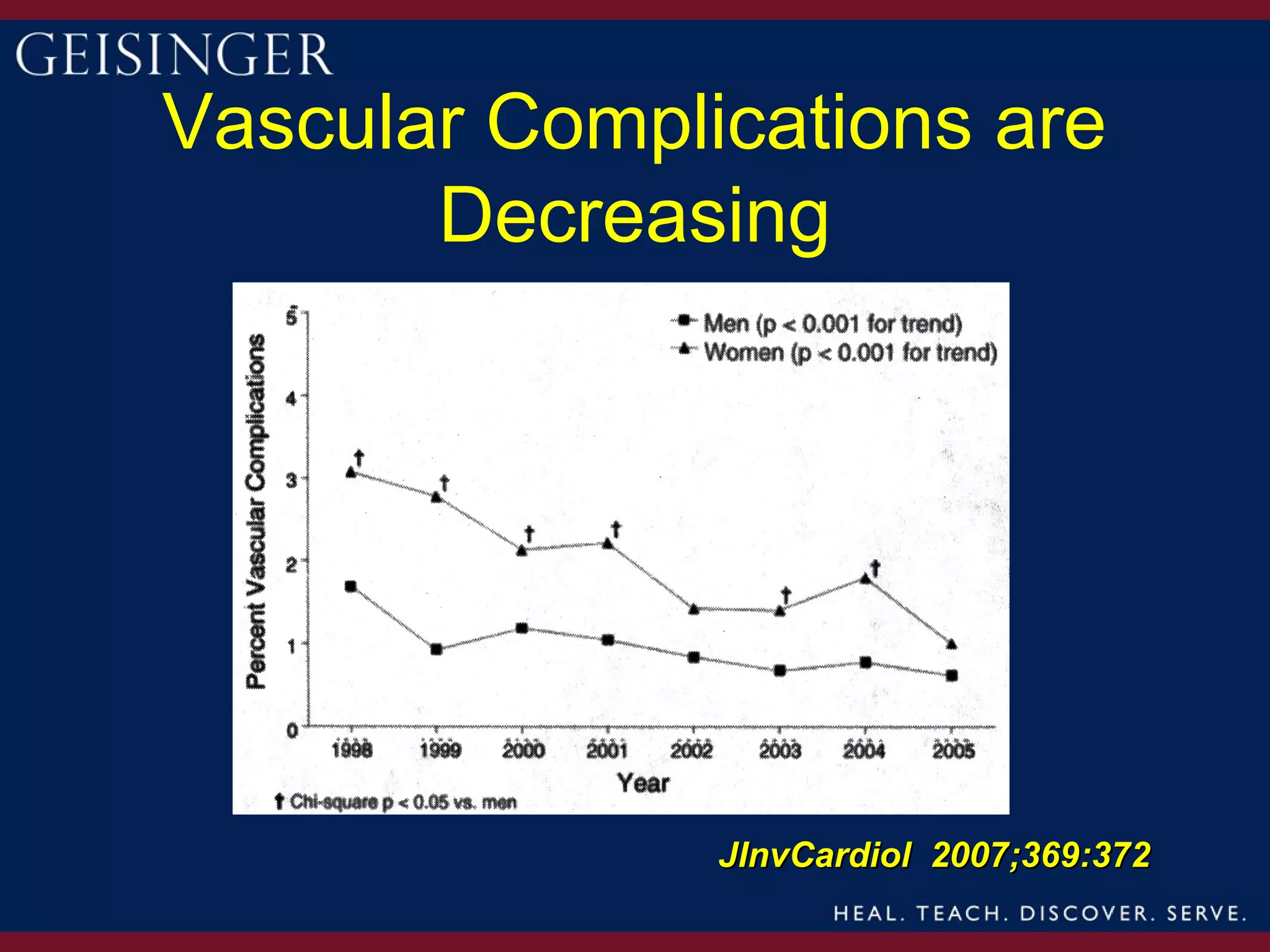
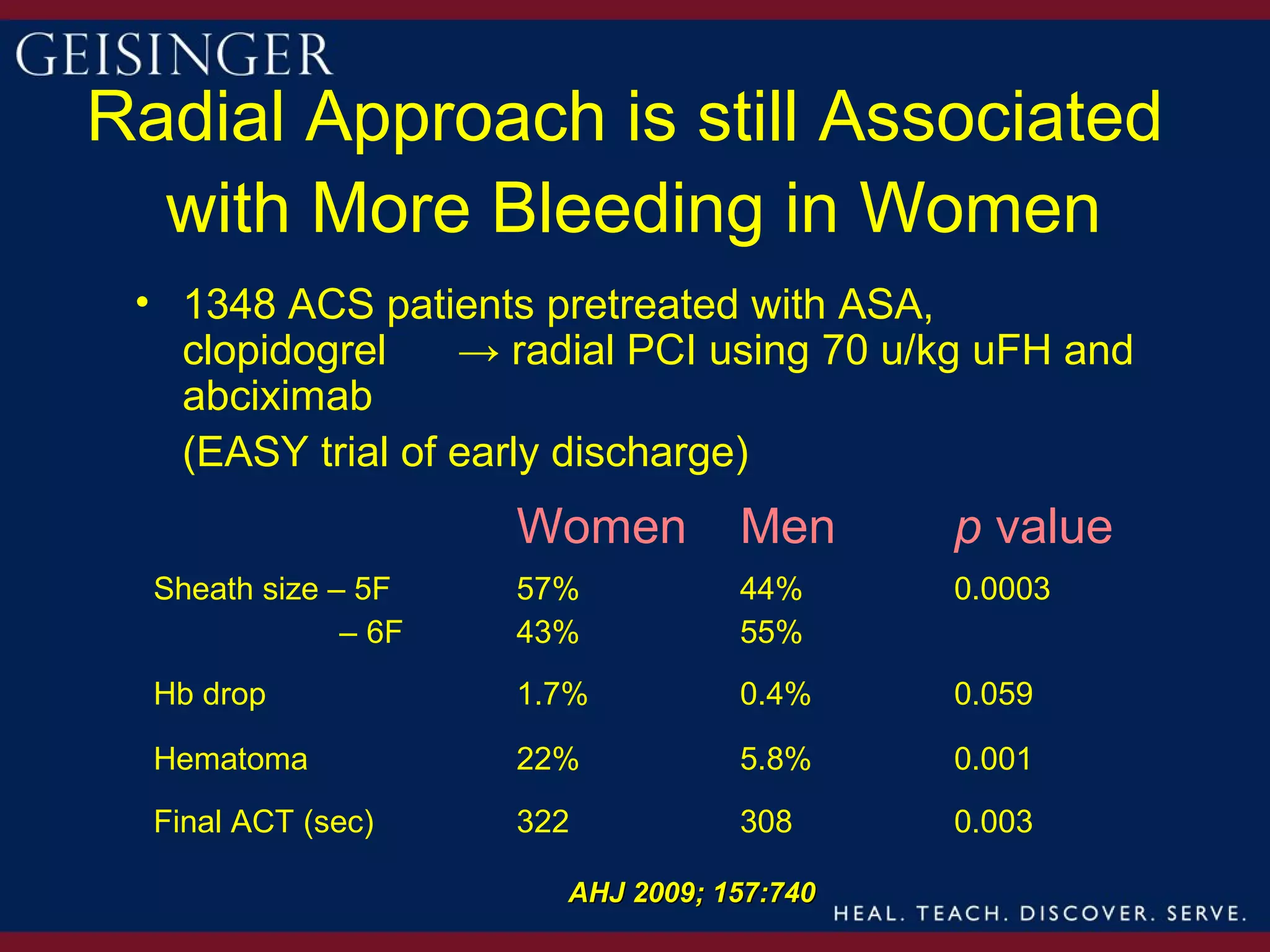
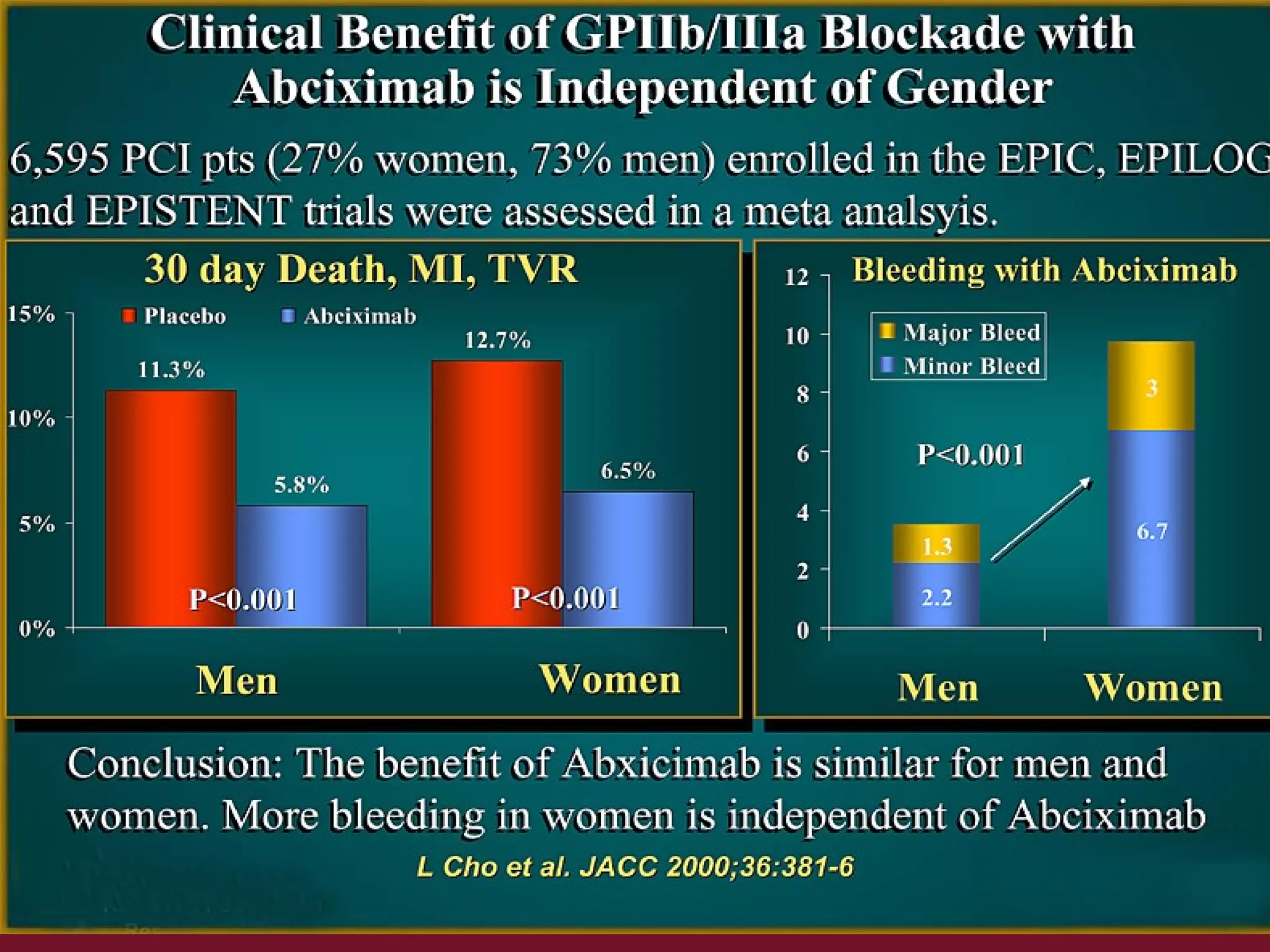


This document provides an overview and update on gender differences in the treatment of acute coronary syndrome (ACS) and percutaneous coronary intervention (PCI). Some key points summarized: 1) Women have historically experienced later referrals for treatment of ACS, resulting in more advanced coronary artery disease and worse outcomes. However, outcomes after PCI have improved over time for both men and women. 2) Women continue to be underrepresented in clinical trials of PCI due to barriers like later presentation and higher risk profiles making them ineligible. 3) While early data showed gender was an independent predictor of mortality after PCI, more recent studies have found no differences in death or re-intervention rates between men and women after adjusting for























































![[Teich] amdis](https://cdn.slidesharecdn.com/ss_thumbnails/teichamdis-131009123653-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Hongsermeier] clinical decision support services amdis final](https://cdn.slidesharecdn.com/ss_thumbnails/hongsermeierclinicaldecisionsupportservicesamdisfinal-131009123754-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)










