Downloaded 159 times







































1. The document discusses the debate around prostate cancer screening in elderly men over age 65, with arguments on both sides. 2. Screening may detect cancers early that would not have progressed or caused harm in a man's lifetime given his life expectancy. However, screening also risks overdiagnosis and overtreatment of biologically unimportant cancers. 3. Guidelines in the US do not recommend routine screening for low-risk, elderly patients due to the scientific uncertainties around the balance of benefits and harms. Patient-clinician discussion is important to make informed, individual decisions.














































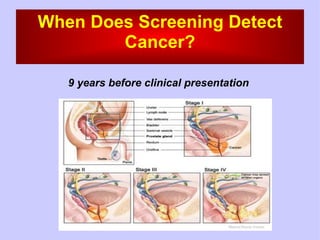
![Ca prostate [edmond]](https://cdn.slidesharecdn.com/ss_thumbnails/caprostateedmond-130318091345-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)







































