
Downloaded 20 times
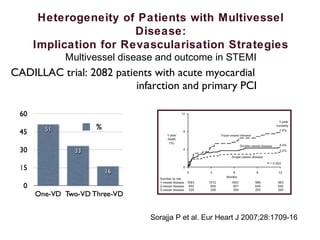
![Heterogeneity of Patients with Multivessel
Disease:
Implication for Revascularisation Strategies
Multivessel disease and outcome in STEMI
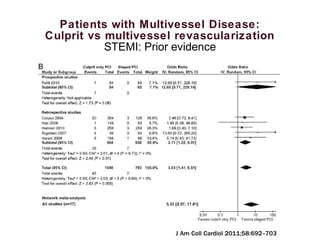
30-Day Mortality for Patients With or Without
Non–Infarct-Related Coronary Artery Disease
4.3% vs 1.7%, risk difference, 2.7%[95%
CI, 2.3%to 3.0%] P < .001
68 765 patients enrolled in 8 trials, 28 282 patients with valid
angiographic data.
Defined as stenosis of 50% or more of a major epicardial artery.
52.8% (14 929) had
obstructive non-IRA
disease:
• 29.6%: 1vessel
• 18.8%: 2 vessels
JAMA. 2014;312(19):2019-2027.](https://image.slidesharecdn.com/josemiguelvegasvallesecsept2015-151001172307-lva1-app6891/85/Jose-miguel-vegas-valle-sec-sept2015-18-320.jpg)
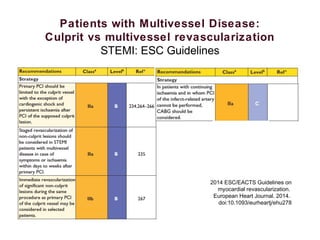
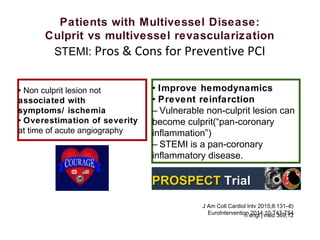
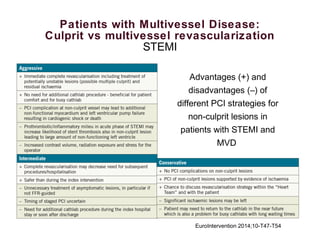

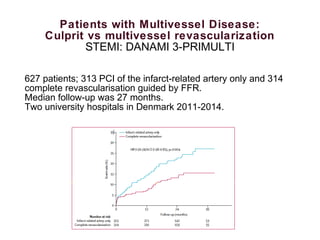
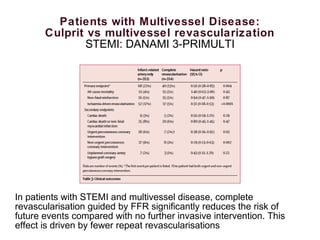
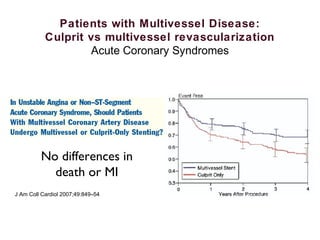
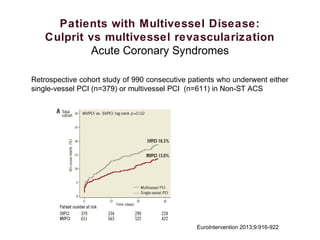
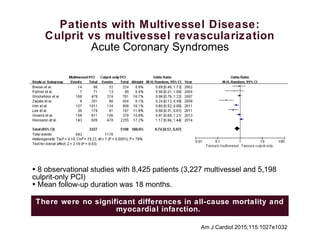

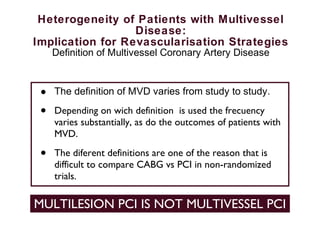
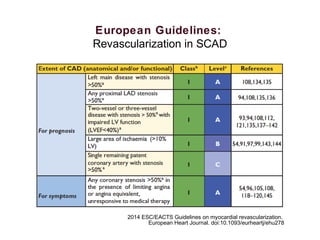
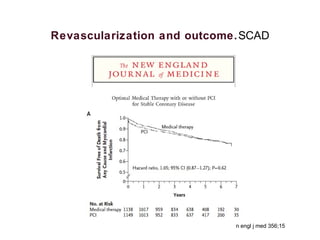
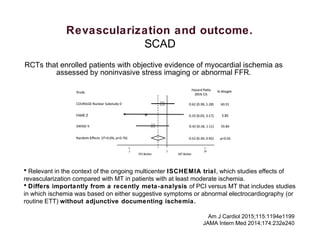
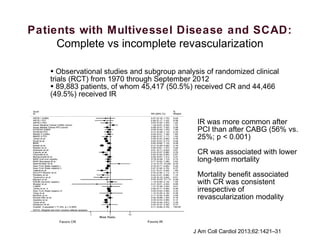
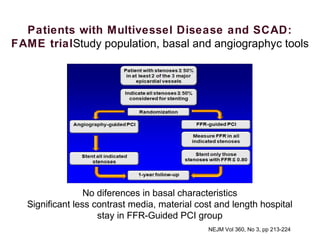
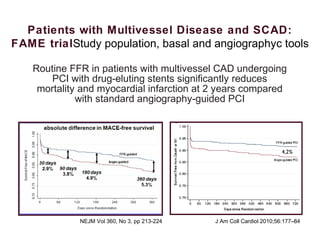
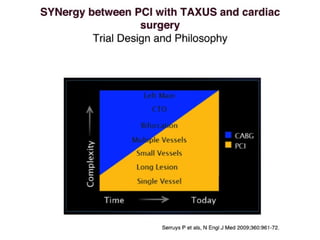
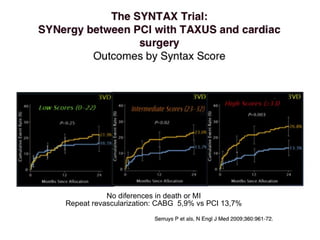
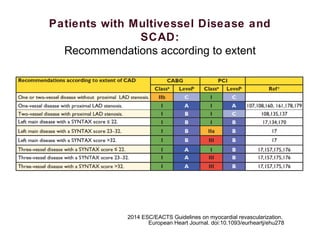
1) Complete revascularization (CR), defined as treating all significant coronary stenoses, is associated with lower mortality compared to incomplete revascularization (IR) based on observational studies and randomized trials. IR is more common after percutaneous coronary intervention (PCI) than coronary artery bypass grafting (CABG). 2) For stable coronary artery disease (SCAD), CR is recommended when feasible, while for acute coronary syndromes (ACS) and ST-segment elevation myocardial infarction (STEMI), treating the culprit lesion only is usually recommended initially, with staged revascularization of non-culprit lesions if needed. 3) Randomized trials of preventive PCI of non-culprit lesions in STEMI























































































