








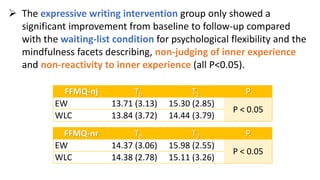
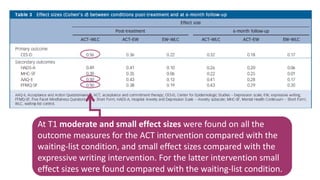
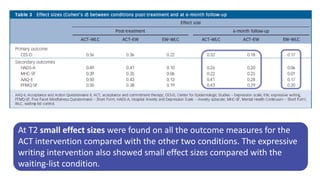
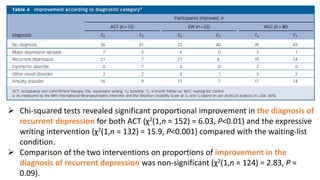
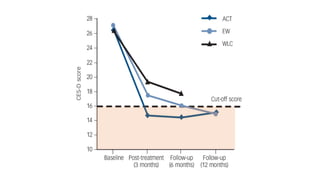



This document outlines a randomized controlled trial evaluating the efficacy of a web-based intervention based on Acceptance and Commitment Therapy (ACT) for reducing depressive symptoms, comparing it with an active control (expressive writing) and a waiting-list group. The study involved adults with mild to moderate depressive symptoms, utilizing various assessments to measure outcomes like psychological flexibility and mental health. Results aimed to contribute to public mental health interventions by addressing recruitment challenges and offering supportive evidence for web-based self-help strategies.



































































