Downloaded 37 times

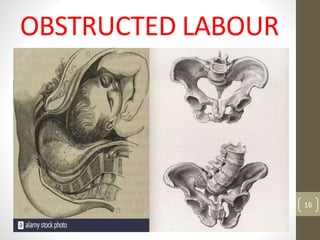



The document discusses obstructed labor and prolonged labor, defining prolonged labor as lasting over 18 hours with specific cervical dilation and descent rates. It outlines the stages of labor, possible causes, management strategies, and the implications for both mother and fetus. Additionally, it emphasizes the importance of early diagnosis and intervention to prevent complications associated with prolonged and obstructed labor.



































































