Downloaded 19 times




![pAO2 from Alveolar Gas Equation
PAO2 =[(PB – PH2O) FiO2 ] – (PaCO2 / RQ)
Atmospheric pressure is 760 mm Hg at sea level
PH2O is vapor pressure of water at 37°C and is equal to 47
mmHg
713 x FiO2 – 1.25 x PaCO2
The respiratory quotient or respiratory coefficient (RQ) is the
ratio of CO2 produced divided by the O2 consumed, and its
value is typically 0.8 (RQ = CO2 eliminated / O2 consumed).
R is taken as 1 @FiO2> 0.6
PB – PH2O is known as PiO2 713
Simplified as
Facebook page: Anesthesia Info from The
PAO2 = 713 x FiO2 – 1.25 x
PaCO2](https://image.slidesharecdn.com/abgflashcards-230326140212-31ae1ea0/85/ARTERIAL-BLOOD-GAS-ANALYSIS-pptx-18-320.jpg)
![The Alveolar –Arterial Oxygen Gradient
PAO2-PaO2
The expected paO2 will be 10-15 mm of Hg lower than that in
the alveoli: A-a O2 gradient
10-15 mm in young to middle aged
PaO2= 109- 0.43 [age in years]
It increases with increase in FiO2 [@FiO2 of 1,110!)
If higher than expected for age, shunt fraction is high
Facebook page: Anesthesia Info from The](https://image.slidesharecdn.com/abgflashcards-230326140212-31ae1ea0/85/ARTERIAL-BLOOD-GAS-ANALYSIS-pptx-19-320.jpg)
![Case Scenario 4
Patient breathing room air, has PaO2 90 mm of Hg, SpO2
96%, and PaCO2 110 mm of Hg. Check the validity (PaO2,
PaCO2 values reliable or not?)
Apply Alveolar Gas Equation
[713x0.2]-[1.2x110]= PAO2 is 18!, but SpO2 is 96. So one
among the value is wrong.
Facebook page: Anesthesia Info from The](https://image.slidesharecdn.com/abgflashcards-230326140212-31ae1ea0/85/ARTERIAL-BLOOD-GAS-ANALYSIS-pptx-23-320.jpg)
![Case Scenario 4
Patient on mechanical ventilation, has PaO2 150 mm of Hg,
FiO2 0.8, and PaCO2 30 mm of Hg. Check the validity and
find the gradient.
Apply Alveolar Gas Equation
[713x0.8]-[1.2x30]= PAO2 is 534. PaO2 is 150. A-a gradient
384
But please remember that the gradient increases with the
FiO2
Facebook page: Anesthesia Info from The](https://image.slidesharecdn.com/abgflashcards-230326140212-31ae1ea0/85/ARTERIAL-BLOOD-GAS-ANALYSIS-pptx-24-320.jpg)
![Case Scenario 5
Patient breathing room air. PaO2 125. PC02 50. Please find
the gradient?
[713x0.2]-[1.2x50]= PAO2 is 86.
PaO2 then cannot be 125
Air bubble?
MESSAGE: Isolated PaO2 value is meaningless without info
about FiO2 and PaCO2- so give enough importance for
’AGE’
Facebook page: Anesthesia Info from The](https://image.slidesharecdn.com/abgflashcards-230326140212-31ae1ea0/85/ARTERIAL-BLOOD-GAS-ANALYSIS-pptx-25-320.jpg)
![CaO2- Oxygen Content
Oxygen carried as oxyhemoglobin + dissolved O2
CaO2= [1.39 X Hb (gm/dl) X Saturation] + 0.003 X PaO2
If Hb=15 g/dl, SaO2 99%, 20.4 ml as oxy Hb + 0.3 ml in
plasma20.7
Anemia: will not affect saturation and evoke physiological
adaptations
Abnormal Hbs will decrease saturation and decrease O2
content; will not affect solubility and so PaO2 will be normal
Facebook page: Anesthesia Info from The](https://image.slidesharecdn.com/abgflashcards-230326140212-31ae1ea0/85/ARTERIAL-BLOOD-GAS-ANALYSIS-pptx-27-320.jpg)
![Key Step: Check for Mixed Venous ‘Hypoxia’!
Decreased Cardiac Output (QT) in the presence of constant
O2 consumption (VO2)
Increased VO2 (shivering, fever)
Decrease mixed venous O2 content: CvO2= (1.39xHbx
SvO2)+(0.003xPvO2)
Normal: SvO2= 75% SvO2 ~ SaO2-[VO2/Hb x QT]
PvO2= 40 mm of Hg
In low CO states with continuing O2 extraction, PvO2 will be
low
Sample from a CVC [if no PAC] can identify low CO states
Facebook page: Anesthesia Info from The](https://image.slidesharecdn.com/abgflashcards-230326140212-31ae1ea0/85/ARTERIAL-BLOOD-GAS-ANALYSIS-pptx-30-320.jpg)

![KEY STEP: ACUTE RESPIRATORY ACID BASE
CHANGES
PaCO2 pH SBE=0
• ACUTE RESPIRATORY ACIDOSIS[
buffering only; 99% in ICF]
PaCO2 pH
• ACUTE RESPIRATORY ALKALOSIS
Facebook page: Anesthesia Info from The](https://image.slidesharecdn.com/abgflashcards-230326140212-31ae1ea0/85/ARTERIAL-BLOOD-GAS-ANALYSIS-pptx-47-320.jpg)

![KEY STEP: FINDING THE ANION GAP
When all the commonly measured anions are substracted
from the cations, the result is a positive value of 12±4 mEq/L
Due to unmeasured anions
Corrected AG = Calculated AG + 2.5 [4.5-measured albumin
in g/dl]
Facebook page: Anesthesia Info from The](https://image.slidesharecdn.com/abgflashcards-230326140212-31ae1ea0/85/ARTERIAL-BLOOD-GAS-ANALYSIS-pptx-55-320.jpg)

![Metabolic Acidosis : effects
Decreased strength of respiratory muscles
Hyperventilation
Myocardial depression
Sympathetic over activity
Decreased arrhythmia threshold
Resistance to catecholamines
Hyperkalemia
Increased metabolic demand [N:5% of VO2; in distress 25%]
Insulin resistance
Facebook page: Anesthesia Info from The](https://image.slidesharecdn.com/abgflashcards-230326140212-31ae1ea0/85/ARTERIAL-BLOOD-GAS-ANALYSIS-pptx-61-320.jpg)
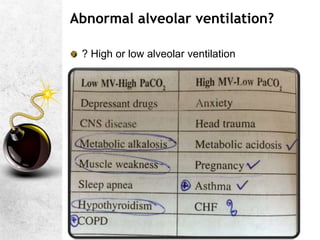
![Metabolic Alkalosis
Generally pCO2 wont go > 55; if > 55, indicates severe
alkalosis OR combined metabolic alkalosis + respiratory
acidosis
Usually [HCO3-] prompt [HCO3-] excretion by kidney;
persistence requires additional process to impair [HCO3-]
excretion](https://image.slidesharecdn.com/abgflashcards-230326140212-31ae1ea0/85/ARTERIAL-BLOOD-GAS-ANALYSIS-pptx-67-320.jpg)
![Additional points- Metabolic alkalosis
Depresses respiration hypoxemia & hypercarbia
Effects on PaCO2 are seen only when HCO3> 35 Mm/L
Chloride responsive [Urinary Cl- < 15 mEq/L]: Rx is chloride-
volume-potassium repletion
Chloride resistant [Urinary Cl- >25 mEq/L]: Rx is correction of
the cause of mineralocorticoid excess and potassium
depletion and Acetazolamide
Facebook page: Anesthesia Info from The](https://image.slidesharecdn.com/abgflashcards-230326140212-31ae1ea0/85/ARTERIAL-BLOOD-GAS-ANALYSIS-pptx-71-320.jpg)

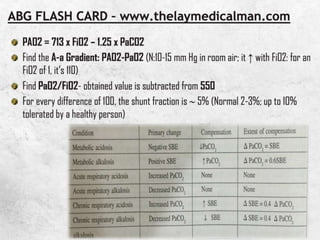
1. An arterial blood gas (ABG) analysis can provide information about oxygenation, ventilation, and acid-base status. It answers questions like how severe hypoxia or hypercarbia is and what acid-base abnormalities may be present. 2. The document provides templates for interpreting ABG results and analyzing acid-base disturbances and their compensation. It also includes several case scenarios where ABG results are used to diagnose conditions like respiratory acidosis from narcotic overdose or metabolic acidosis and hyperventilation from pneumonia. 3. Key steps in ABG interpretation involve checking for hypoxemia and quantifying any shunt fraction, evaluating ventilation and dead space, identifying primary acid-base disturbances and compensation











































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









