Download to read offline





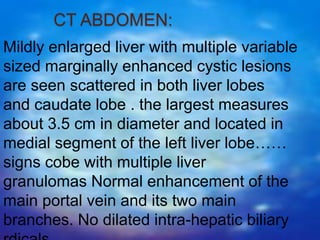

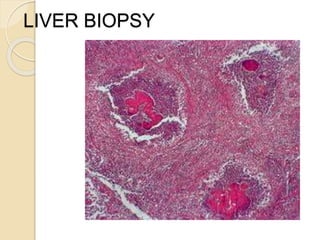

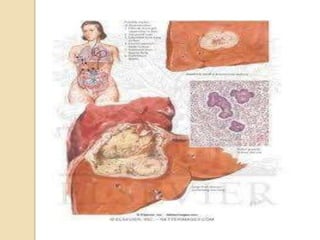
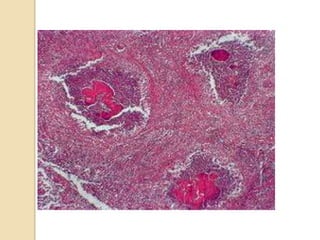

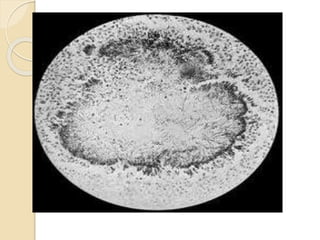
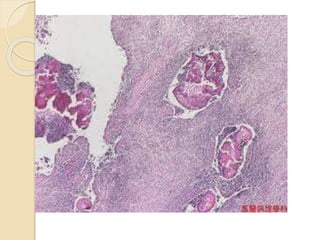



This document summarizes a case study of a 65-year-old female patient who presented with fever, headache, abdominal discomfort and weight loss for 3 months. Imaging revealed multiple liver lesions and biopsy identified the bacteria Actinomyces israelii. The patient was treated with antibiotics and drainage of liver abscesses, leading to complete resolution of symptoms. Actinomycosis is a rare infection caused by Actinomyces bacteria that can form liver abscesses. Diagnosis requires biopsy and culture, while treatment involves prolonged antibiotics and drainage of affected areas.






























































































