Downloaded 18 times



















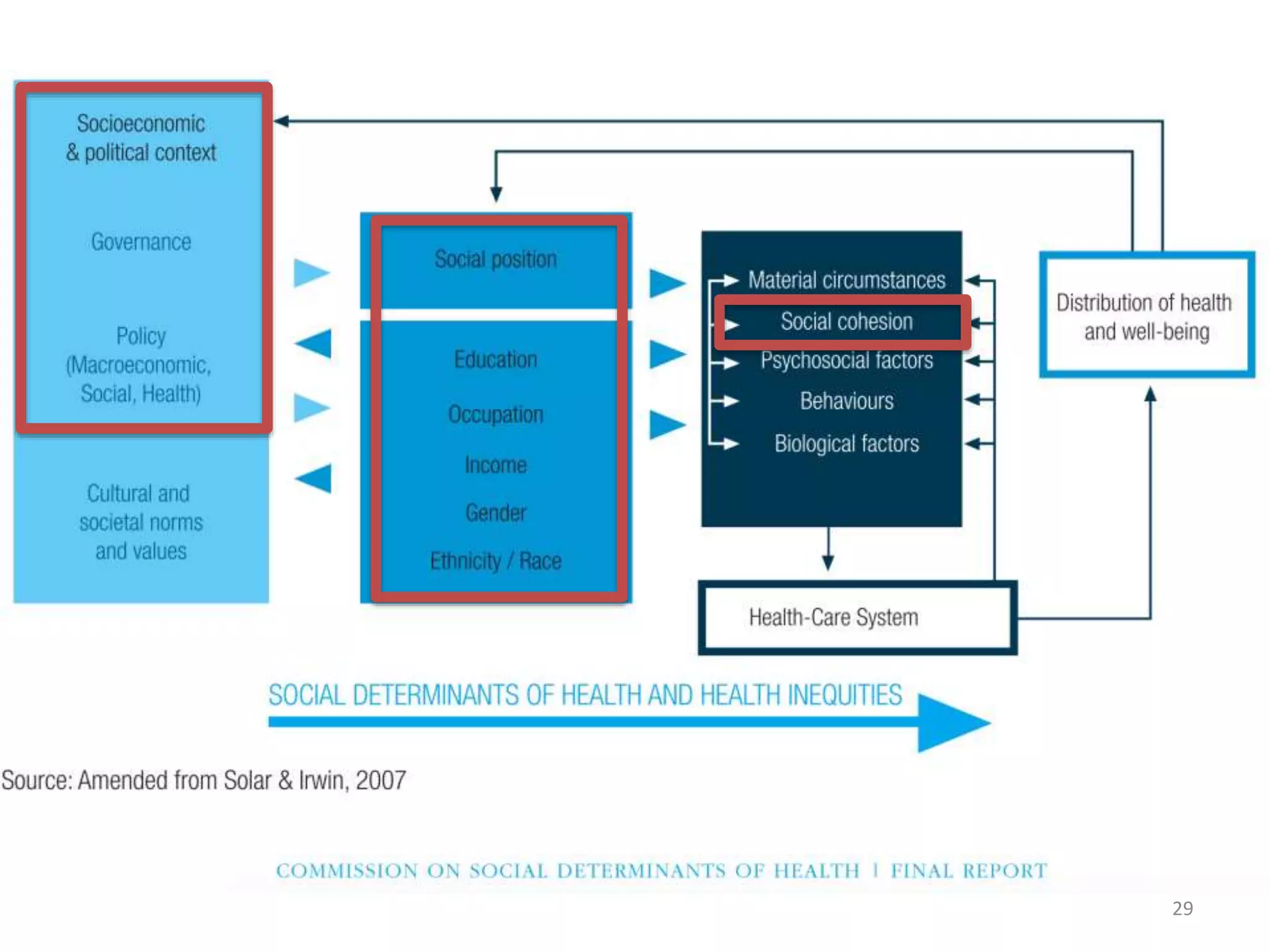














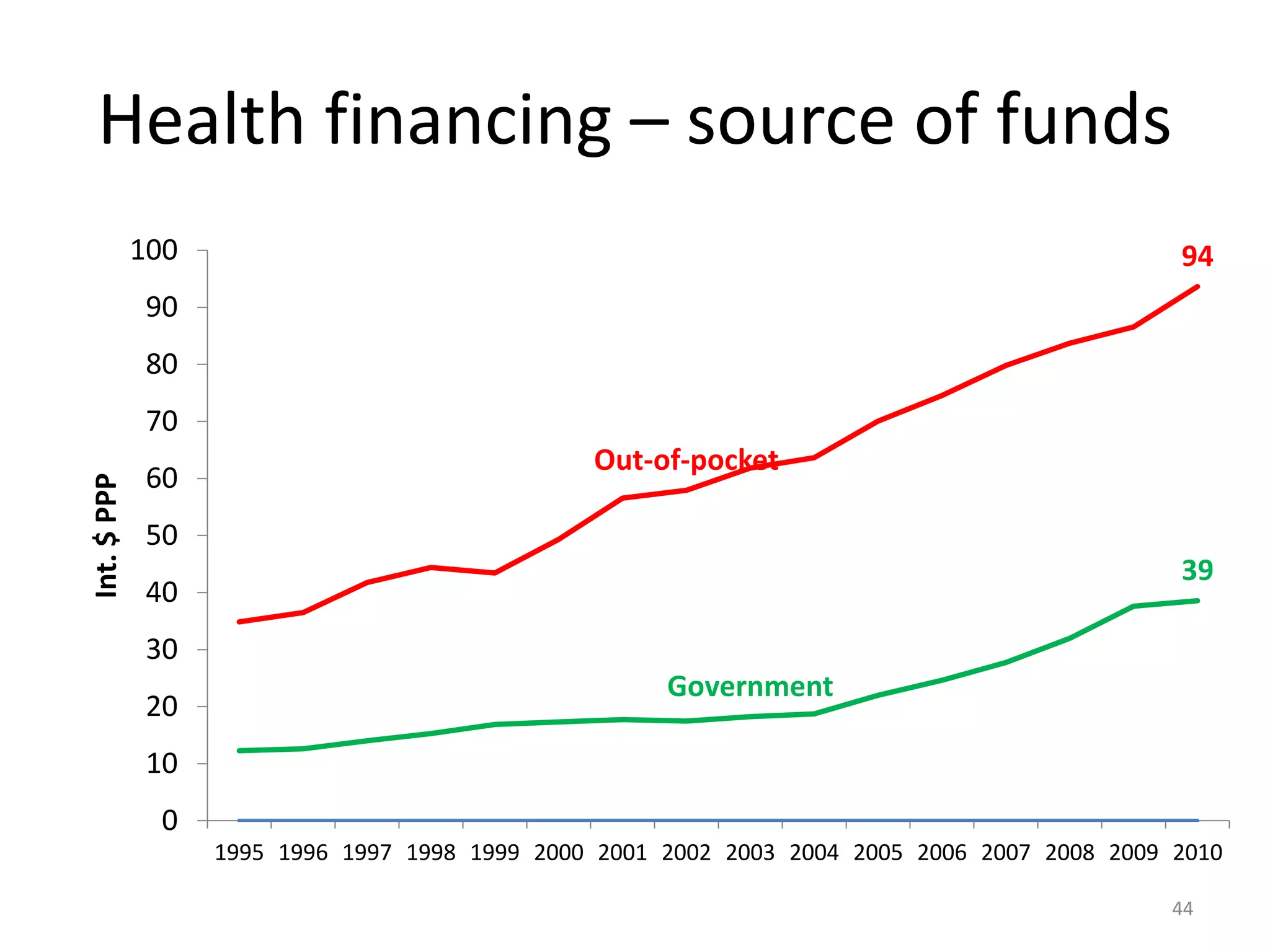




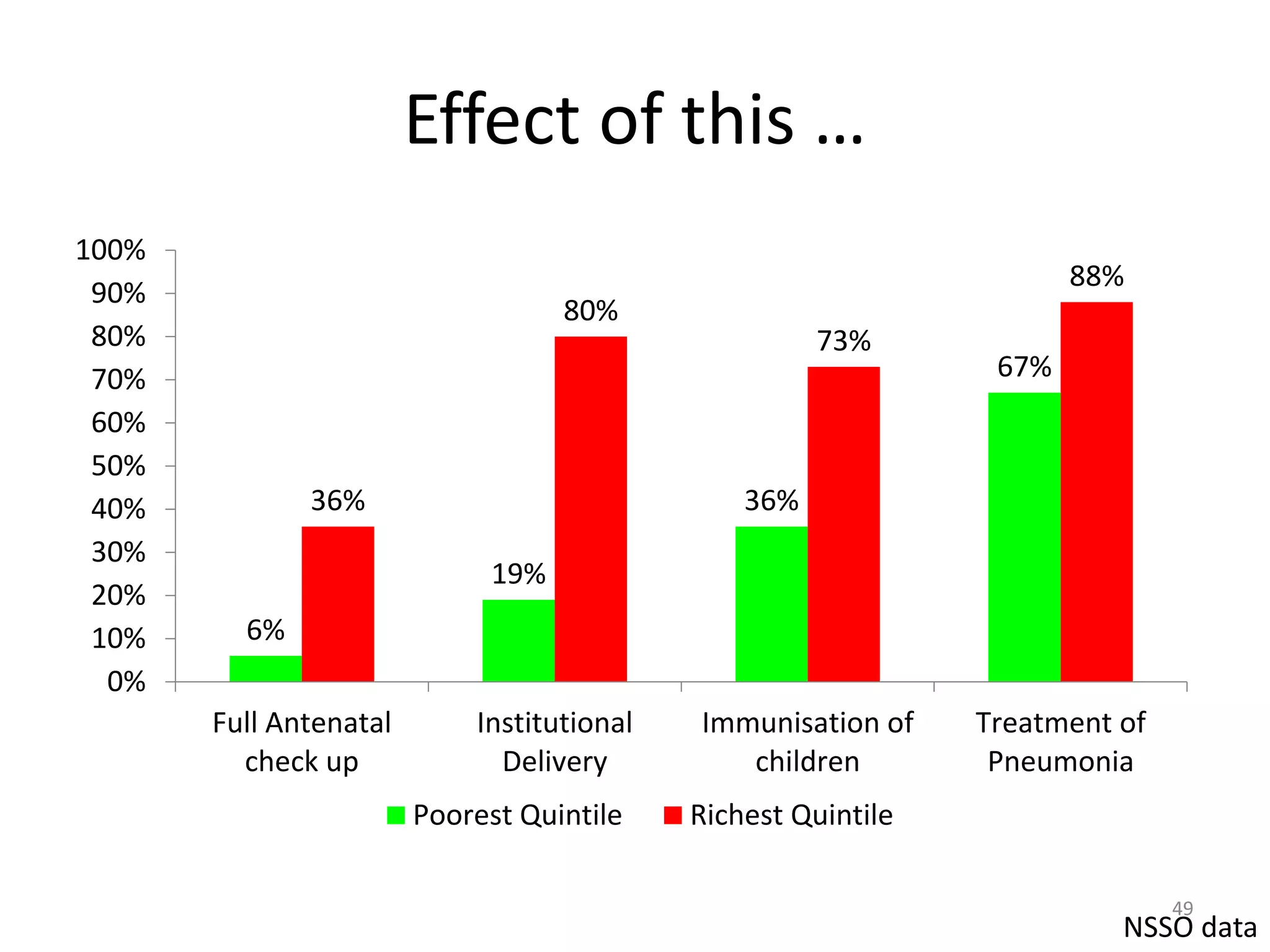
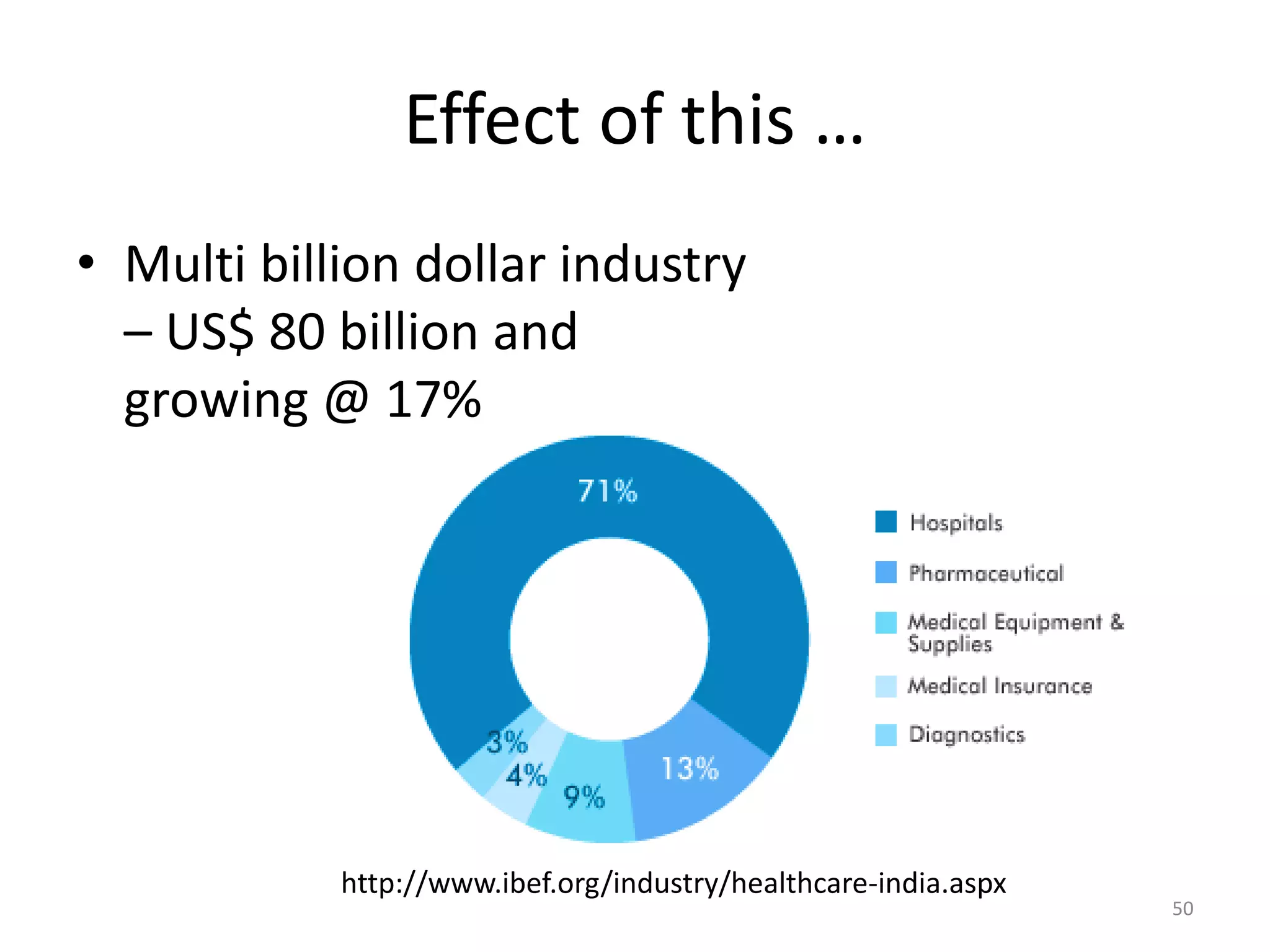


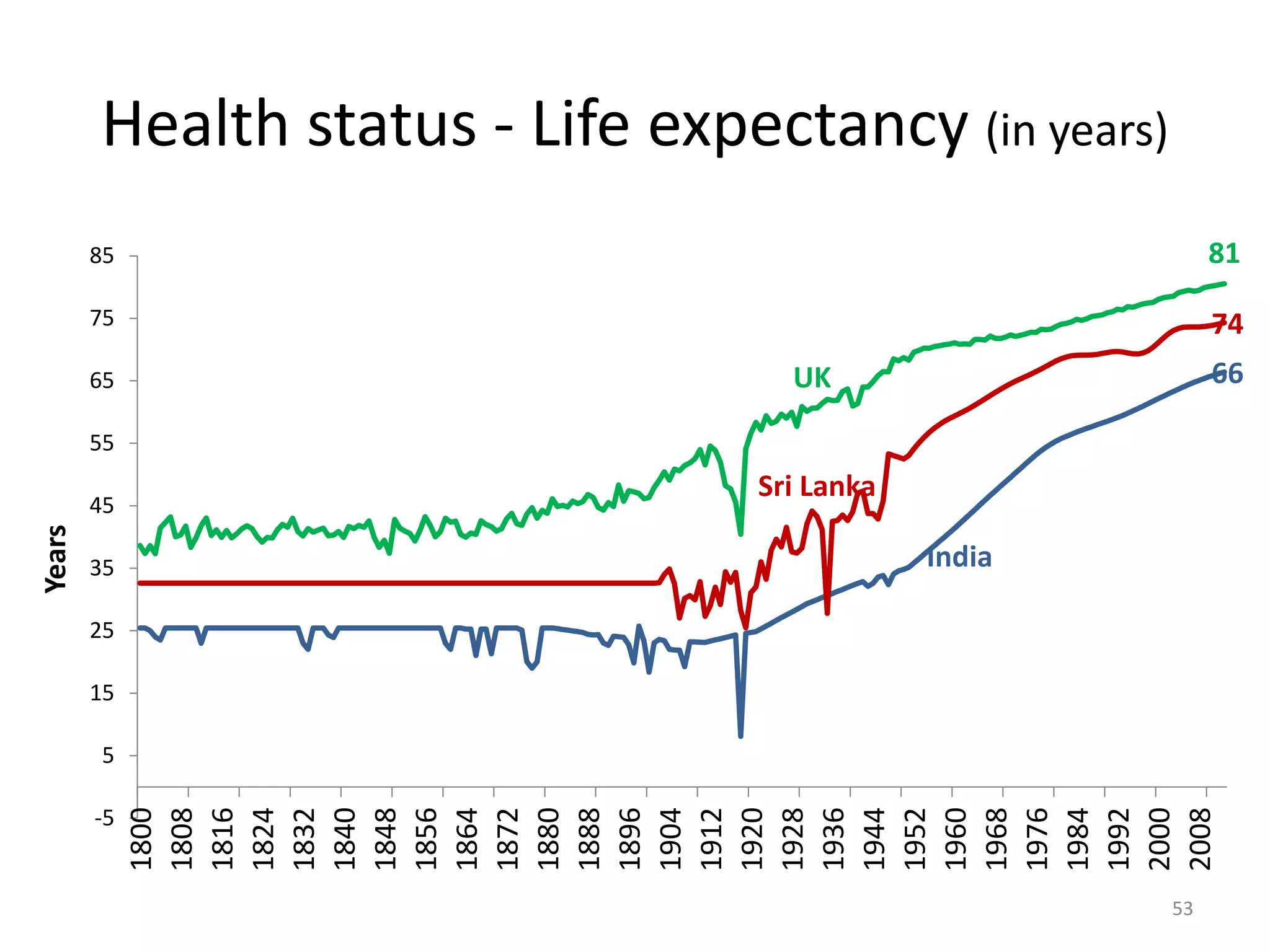




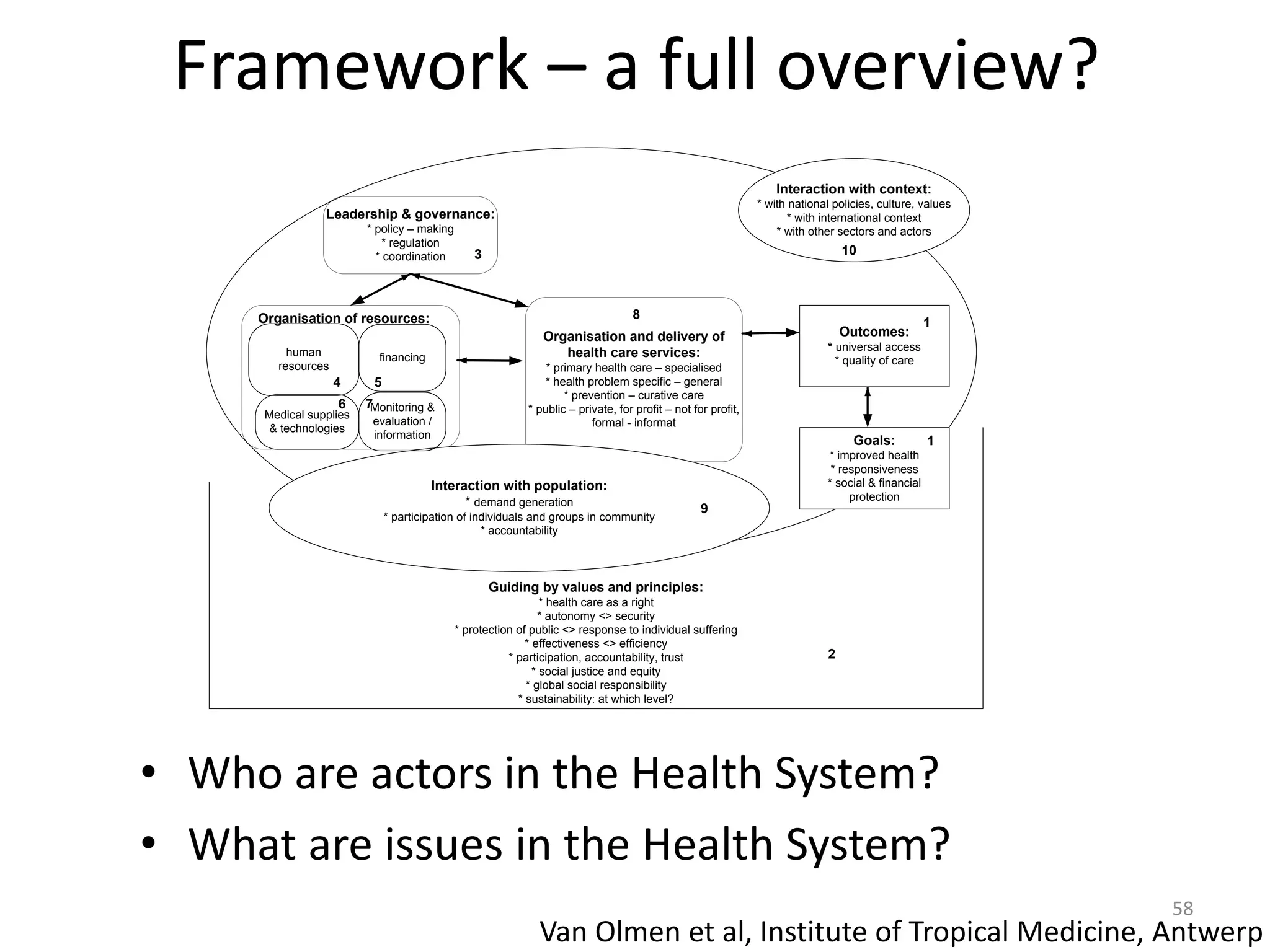


The document provides an overview of the Indian health system, addressing issues such as healthcare inequity, human resource challenges, financing models, and the dual burden of communicable and non-communicable diseases. It highlights the complex landscape of health services in India, characterized by a strong private sector and significant out-of-pocket expenses for patients. The analysis includes social determinants of health and the need for improved governance and efficiency in health expenditure by the government.























































































