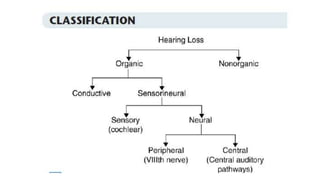
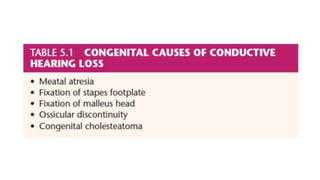
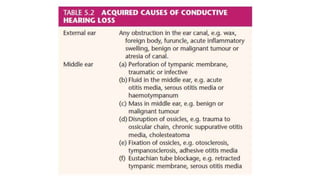
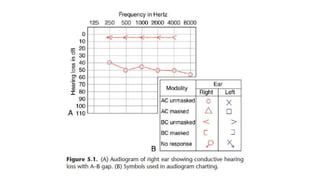
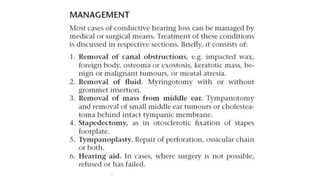
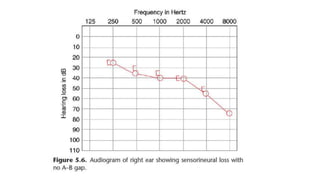
This document summarizes different types and causes of deafness. It discusses conductive hearing loss, which results from issues in the external ear, middle ear, or ear bones. Sensorineural hearing loss affects the inner ear or auditory nerve. Mixed hearing loss has both conductive and sensorineural components. Common causes of sensorineural hearing loss include genetic factors, noise exposure, certain medications, autoimmune disorders, sudden hearing loss, presbycusis, and nonorganic hearing loss. The document also covers deafness in children, which can have prenatal, perinatal, or postnatal causes such as genetic anomalies, infections, complications of prematurity, birth injuries, or postnatal illnesses/medications. Assessment methods like