Mechanical injury refers to tissue damage caused by mechanical force. This chapter discusses the classification and types of mechanical injuries including:
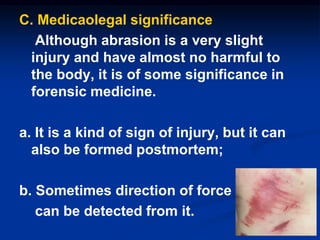
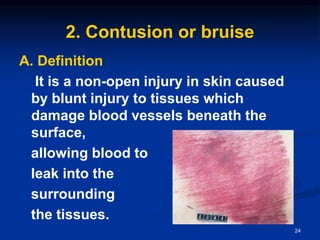
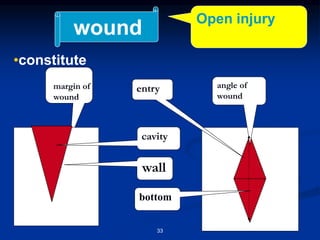
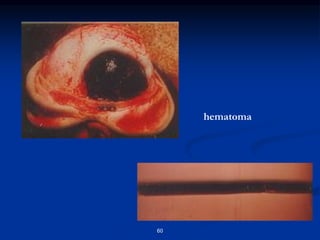
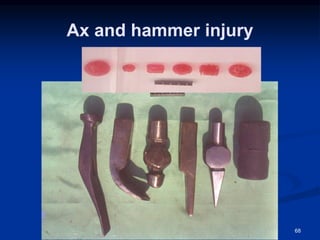
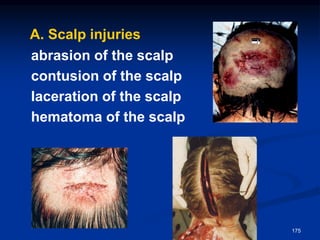
1) Abrasions which destroy the epithelial skin layer from rough impact. Contusions cause bleeding beneath the skin from blunt force. Wounds are open injuries to skin and organs from greater blunt or sharp force.
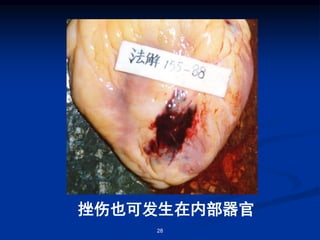
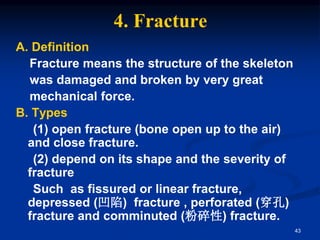
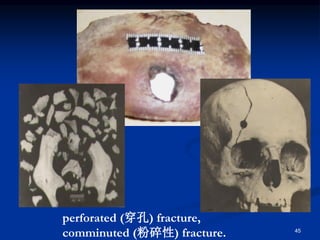
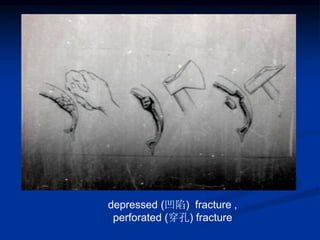
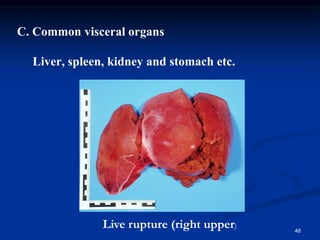
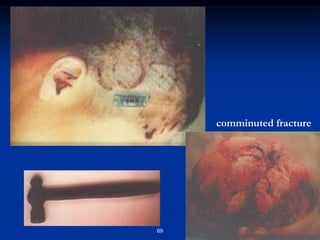
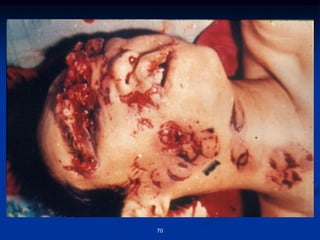
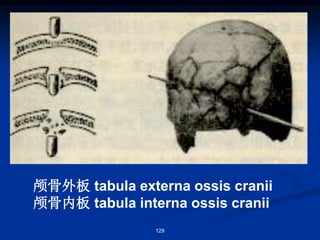
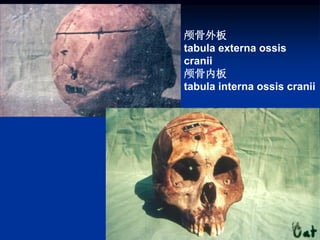
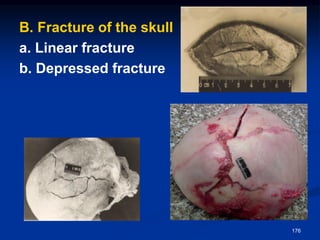
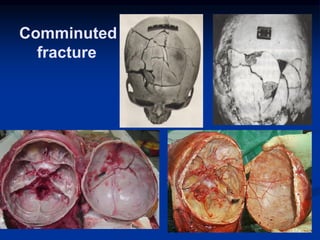
2) Fractures break bone structure from very strong force. Visceral ruptures destroy internal organ integrity. Fragmentation severely damages parts of the body often lethally.
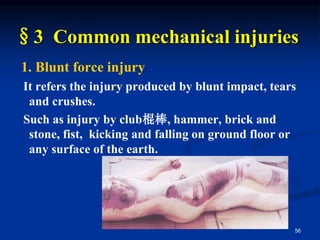
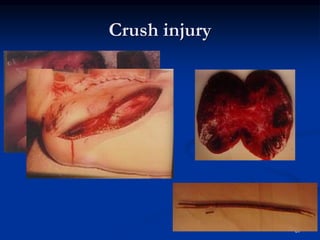
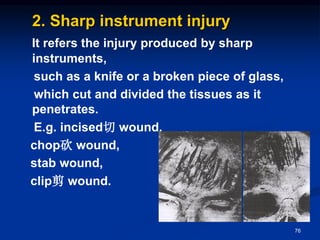
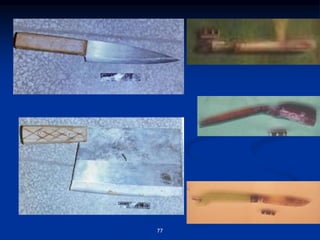
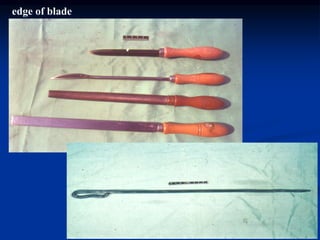
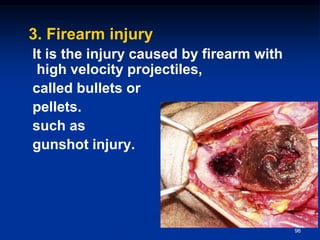
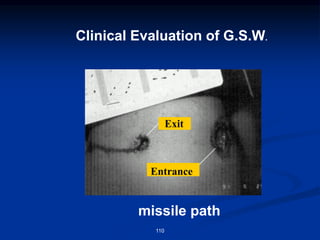
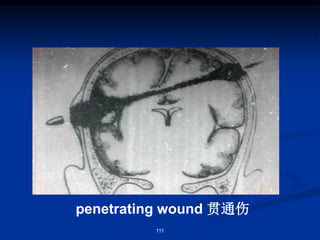
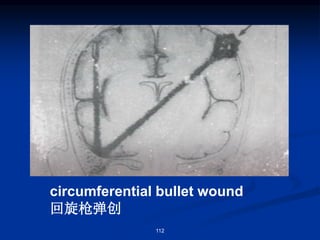
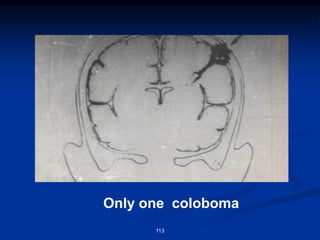
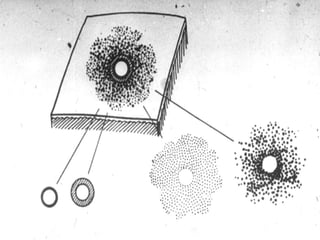
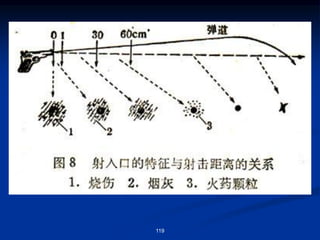
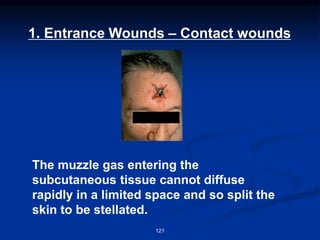
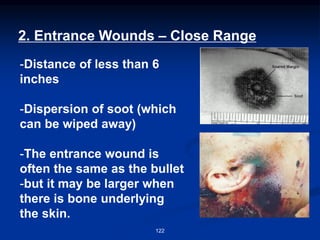
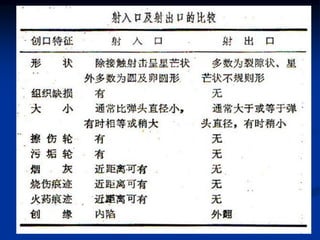
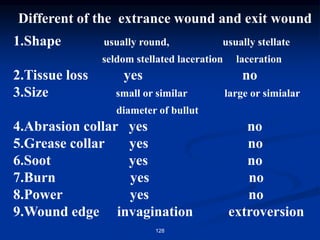
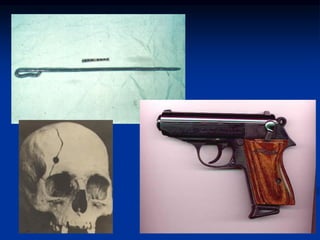
3) Common injuries include blunt injuries from objects like fists or sticks, and sharp injuries from knives or firearms which have distinguishing wound features. Crush injuries compress and intensely damage body surfaces.



























































![[Forensics] traumatology 2.ppt](https://cdn.slidesharecdn.com/ss_thumbnails/forensicstraumatology2-150502144307-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)





![[Forensics] traumatology 1](https://cdn.slidesharecdn.com/ss_thumbnails/forensicstraumatology1-150502144040-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)

























































