Downloaded 50 times

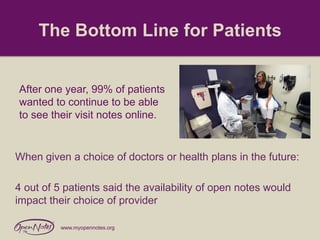


OpenNotes began as a research project that studied the effects of allowing patients access to their primary care doctors' visit notes. The study found that patients who read their notes felt more engaged in their care, better understood their conditions, and were better prepared for visits. Doctors had initial concerns about increased workload, but found little real impact. After one year, 99% of patients and the majority of doctors wanted to continue open notes access. The research demonstrated that open notes can help patients manage their health more effectively with little negative impact. The open notes movement has now expanded beyond primary care and many organizations are adopting the practice.






















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















