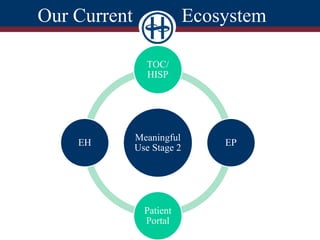
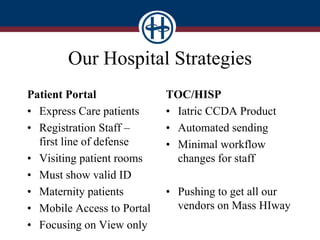
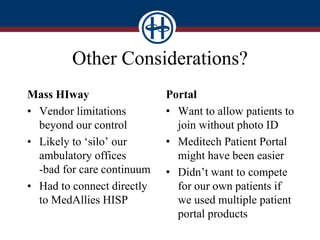
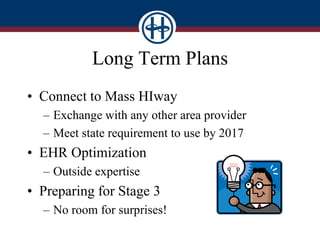
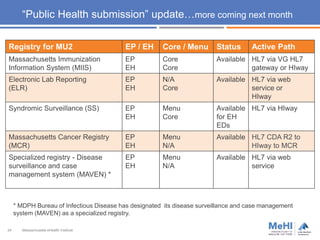
The document outlines the goals and measures of Meaningful Use Stage 2 (MU2), emphasizing interoperability and health information exchange (HIE) in the context of transitions of care and patient access to health information. It details specific objectives for eligible providers and hospitals, including the provision of summary care records and patient access to their health data. Furthermore, it addresses strategies for engaging with HIE partners and highlights the status and submission pathways for public health registries in Massachusetts.



















![New clinical quality measure reporting in Practice Fusion [slides]](https://cdn.slidesharecdn.com/ss_thumbnails/junecqmwebinarslideshare-140611132004-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)