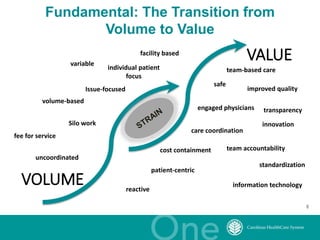
The document discusses the challenges and opportunities in transitioning from a volume-based to a value-based healthcare system at Carolinas Healthcare System, which consists of 39 hospitals and over 30,000 employees. It emphasizes the importance of integrated care models, technology, and accountability in improving patient outcomes and reducing costs. The presentation outlines a maturity model for integration and highlights achievements in patient care and safety through various initiatives.









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
