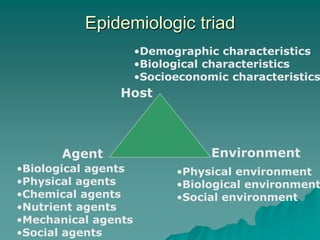
This document provides definitions and concepts related to communicable disease epidemiology. It defines epidemiology as the study of health-related states and events in populations. The epidemiologic triad shows the interaction between host, agent, and environment. A communicable disease is an illness transmitted directly or indirectly between humans, animals, or the environment. Studying communicable disease epidemiology is important for understanding changes in disease patterns, discovering new infections, and investigating chronic disease origins. Key concepts covered include reservoirs, modes of transmission, susceptible hosts, outbreak definitions, and the chain of infection.