Adenoviruses…
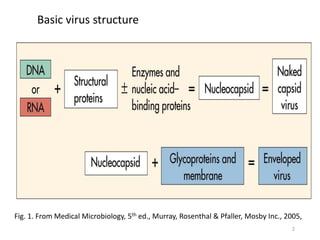
Classification & structure:
Family:Adenoviridae
First isolated in 1953 in a human adenoid cell culture.
ds DNA Genome, Non - enveloped
More than 49 human stereotypes known
Common stereotypes: 1 -8, 11, 21, 35, 37, 40 & 41
►Types 40 & 41 are enteric pathogens
10
11.
Adenoviruses…
• General Properties
•Not easily affected by:
External environment
Low PH
Bile salts & proteolytic enzymes
Can replicate to high titer in the gastro intestinal tract
• 70-90 nm in size
• Linear ds DNA genome with core proteins
11
Time-course of infection
•Incubationperiod- 2-14 days
• Infective period continues for weeks
• Intermittent and prolonged rectal shedding
• Secondary attack rate within families up to
50%
14
15.
Pathogenesis and Immunity
•Capableof causing
• Lytic (e.g., mucoepithelial cells),
• Latent (e.g., lymphoid and adenoid cells),
• Transforming (hamster, not human) infections.
• The viral fiber proteins determine the target
cell specificity.
16.
Epidemiology
• Resist drying,detergents, gastrointestinal tract
secretions (acid, protease, and bile), and even
mild chlorine treatment.
• Can be spread by the fecal-oral route, by fingers,
by fomites (including towels and medical
instruments), and in poorly chlorinated swimming
pools.
17.
Epidemiology
• Are spreadmainly by respiratory or fecal-oral contact
from human to human.
• Close interaction among people, as occurs in classrooms
and military barracks, promotes spread of the virus.
• Most infections are asymptomatic, a feature that greatly
facilitates their spread in the community.
• Adenoviruses 1 through 7 are the most prevalent
serotypes
18.
Adenoviruses…Clinical syndrome
Different basedon organ or system involved
1. Respiratory system
• Upper respiratory infections: common cold
(rhinitis) ; pharyngitis & tonsillitis
• Lower respiratory infections: bronchitis &
pneumonia
18
19.
Adenoviruses…
2. Eye
• Acutefollicular conjunctivitis & Kerato Conjunctivitis
3. Gastrointestinal
Gastroenteritis
Diarrhea tends to last longer than other viruses that cause
Gastroenteritis E.g. Rotavirus
4. Mesenteric adenitis ; hepatitis ; appendicitis
• May cause fatal disease in immuno-compromised
patients
19
20.
• Diagnosis
• Culture,viral antigen detection
• Treatment
Live military vaccine
• Live virus vaccine containing serotypes 4 and 7,
enclosed in enteric-coated capsules and
administered orally, has been used in military
recruits
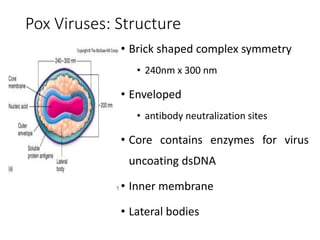
• Pox Viruseshave been known - the characteristic
"pocks" produced by variola virus (Smallpox) .
• Largest and most complex
• Similar morphologically, share a common
nucleoprotein antigen
• Infection characterized-skin rash
22
POXVIRUSES
23.
• Largest, mostcomplex viruses
• First animal virus seen microscopically
• First virus grown in tissue culture
• DNA Viruses that replicate in cytoplasm
• Encodes all transcription and replication enzymes
needed for viral genome
• First virus Physically purified
23
Properties of Poxviruses
24.
•First virus Chemicallyanalyzed
•Small pox first disease eradicated
At least 9 different poxviruses cause disease
in humans,
but variola virus (VV) and vaccinia are the
best known.
24
Properties of Poxviruses con’t
25.
25
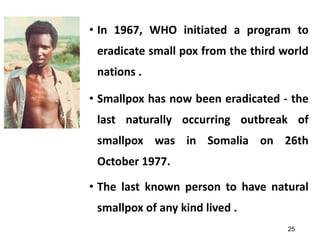
• In 1967,WHO initiated a program to
eradicate small pox from the third world
nations .
• Smallpox has now been eradicated - the
last naturally occurring outbreak of
smallpox was in Somalia on 26th
October 1977.
• The last known person to have natural
smallpox of any kind lived .
26.
26
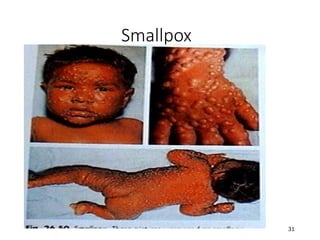
Clinical Features ofHuman Poxviruses
• Smallpox is caused by two strains of the same
virus:
• Variola major - more common, causes a severe form
of the disease
• Mortality rate of 15 – 30%
• Variola minor - causes a mild form of disease
• 1 - 2% mortality rate
Variola (smallpox)
27.
27
Transmission
• Person Person
• Primarily droplet, or aerosol
• smallpox in droplet nuclei can live between a few
hours and a few days in the environment
• No animal reservoir or vector
• Very contagious
• Persons are very sick before contagious
28.
28
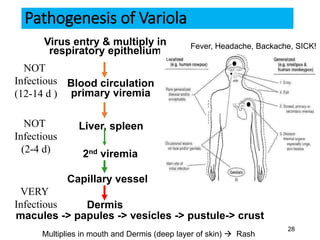
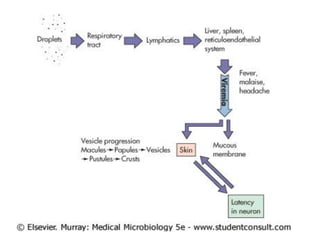
Pathogenesis of Variola
Virusentry & multiply in
respiratory epithelium
Blood circulation
primary viremia
Liver, spleen
2nd viremia
Capillary vessel
Dermis
macules -> papules -> vesicles -> pustule-> crust
Fever, Headache, Backache, SICK!
NOT
Infectious
(12-14 d )
NOT
Infectious
(2-4 d)
Multiplies in mouth and Dermis (deep layer of skin) Rash
VERY
Infectious
29.
29
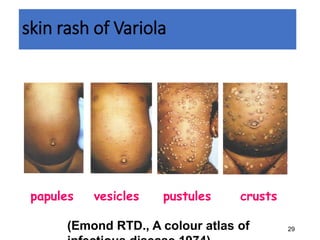
skin rash ofVariola
papules vesicles pustules crusts
(Emond RTD., A colour atlas of
32
Other Poxvirus Infections
•Poxvirus infections also occur in animals
• Transmission to humans requires contact with
infected animals
• Infections of humans are usually mild
• Can result in pox and scars but little other
damage
• Edward Jenner used cowpox to immunize
individuals against smallpox
Edward Jenner (1749-1823)
33.
33
Monkeypox
• In humans,monkeypox is similar to smallpox, although it is often
milder.
• Unlike smallpox, monkeypox causes lymph nodes to swell
(lymphadenopathy).
• Within 1 to 3 days (sometimes longer) after the appearance of
fever, the patient develops a papular rash (i.e., raised bumps),
often first on the face but sometimes initially on other parts of
the body.
• The illness typically lasts for 2 to 4 weeks.
• Human monkeypox is believed to have a fatality rate of 1% to 10%.
35
Smallpox Eradication
• Whywas smallpox (variola) a good candidate for eradication?
• Variola has a narrow host range.
• There are no carriers.
• There are no animal reservoirs.
• A highly effective an inexpensive freeze-dried vaccine was
available.
• Surveillance of the disease was easy (centrifugal rash).
• The WHO created a program to eradicate it.
• WHO commitment 1967 →Eradication 1980
36.
36
Bioterrorism or Re-emergence?
•Although smallpox has been eradicated, there are
concerns about the potential use of variola virus as a
weapon of terror.
• Use of variola as a biological weapon has a long history.
• Variola as germ warfare against Native American Indians,
French and Indian Wars (1754 - 763).
• Consequently, destruction of the last (official) remaining
smallpox stocks held in Russia and USA has now been
postponed indefinitely.
37.
37
Bioterrorism or Re-emergence?
•The possibility of an orthopoxvirus such as variola,
monkeypox, camelpox or taterapox virus emerging or
re-emerging as a threat to human health increases .
• Finally, it is unclear whether all, only a few, or just one of
the differences between the genomes of viruses such as
camelpox and smallpox.
• Genetic modification of camelpox to delete genes that
are present in camelpox but absent in smallpox might be
highly dangerous.
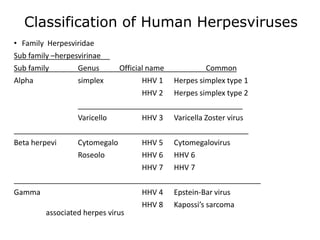
Classification of HumanHerpesviruses
• Family Herpesviridae
Sub family –herpesvirinae
Sub family Genus Official name Common
Alpha simplex HHV 1 Herpes simplex type 1
HHV 2 Herpes simplex type 2
________________________________________
Varicello HHV 3 Varicella Zoster virus
_________________________________________________________
Beta herpevi Cytomegalo HHV 5 Cytomegalovirus
Roseolo HHV 6 HHV 6
HHV 7 HHV 7
____________________________________________________________
Gamma HHV 4 Epstein-Bar virus
HHV 8 Kapossi’s sarcoma
associated herpes virus
41.
Herpes virus…..
• Capacityto persist in host indefinitely in nucleus of
the cell
• Varicella zoster and herpes simplex viruses establish latent
infections in neurons
• CMV , EBV and HHV-6 : persist in lymphocytes
• Reactivation are more likely to take place during
periods of immunosuppression.
• Both primary infection and reactivation are likely to be
more serious in immunocompromised patients.
42.
Herpes virus Virion
•Spherical 150- 250 nm Icosahedral
• ds DNA linear 124-235 kbp
• More than 35 proteins in virion
• Envelope: 8nm spikes viral glycoproteins. Fc receptors.
• Replication nuclear, bud from nuclear membrane
• Infection: Lytic, latent and recurrent
• Common Antigens: None!
43.
1. Herpes SimplexViruses (HSV)
• Extremely widespread in the human population.
• Responsible for a spectrum of diseases
• Gingiva-stomatitis
• Kerato-conjunctivitis
• Encephalitis
• Genital disease and infections of newborns.
• The HSV establish latent infections in nerve cells;
recurrences are common
44.
Properties of theViruses
• are two distinct HSVs: (HSV-1, HSV-2).
• Their genomes are similar in organization
• They can be distinguished by sequence analysis of viral
DNA.
• The two viruses cross-react serologically.
• They differ in their mode of transmission
• HSV-1 is spread by contact, usually involving infected saliva
• HSV-2 is transmitted sexually or from a maternal genital infection
to a newborn.
45.
Characteristics
HSV causes cytolyticinfections
Lesions induced in the skin and mucous membranes.
Characteristic histopathologic changes include
• ballooning of infected cells
• production of intranuclear inclusion bodies
• formation of multinucleated giant cells.
• Cell fusion provides an efficient method for cell-to-cell
spread of HSV, even in the presence of neutralizing
antibody.
46.
p
a
g
e
5
4
4
Disease Mechanisms forHerpes Simplex Viruses
p
a
g
e
5
4
4
1. Disease is initiated by direct contact and depends on
infected tissue (e.g., oral, genital, brain).
2. Virus causes direct cytopathologic effects.
3. Virus avoids antibody by cell-to-cell spread (syncytia).
4. Virus establishes latency in neurons (hides from
immune response).
5. Virus is reactivated from latency by stress or immune
suppression.
6. Cell-mediated immunopathologic effects contribute to
symptoms.
47.
Epidemiology of HerpesSimplex
• HSV1 is transmitted by kissing or other contact with
saliva
• HSV2 is spread by sexual contact
• HSV2 is spread nosocomially
48.
Primary Infection
• HSV-1infections are limited to the oropharynx, and virus
is spread by respiratory droplets or by direct contact with
infected saliva.
• HSV-2 is usually transmitted by genital routes.
• Virus then invades local nerve endings and is transported
by retrograde axonal flow to dorsal root ganglia, where,
after further replication, latency is established.
49.
Primary Infection
•HSV-1 infectionsresult in latent infections
in the trigeminal ganglia
•HSV-2 infections lead to latently infected
sacral ganglia.
•Primary HSV infections are usually mild;
most are asymptomatic.
50.
Genital Herpes
• Genitalherpes is characterized by vesiculo-
ulcerative lesions of the penis of the male or of the
cervix, vulva, vagina, and perineum of the female.
• The lesions are very painful and may be associated
with fever, malaise, dysuria, and inguinal
lymphadenopathy.
• Viral excretion persists for about 3 weeks.
51.
Neonatal Herpes Simplex
•Infants acquire the virus passing through the
birth canal.
• Disseminated herpes - newborns; premature
infants susceptible
52.
Treatment HSV1
• Thefirst drugs were used to treat conjunctivitis and
keratitis
• Iododeoxyuridine
• Trifluridine
• Adenine arabinoside
• Acyclovir
53.
Treatment HSV1
• Iododeoxyuridine:direct application to the cornea
• Trifluridine, Keratitis: direct application
• Adenine arabinoside: direct application to the
cornea. Intravenously injected, it reduces mortality
from herpes encephalitis.
• Acyclovir: is now the drug of choice, is the least toxic.
Can be used topically, orally and intravenously.
54.
Treatment HSV2
• Acyclovirdoes not cure the initial infection, but
because it prevents the attachment of released
virus from an infected cell, it ameliorates the
disease.
• With aggressive treatment eventually the viruses
disappear.
• It is not an effective cure for the latent stage.
55.
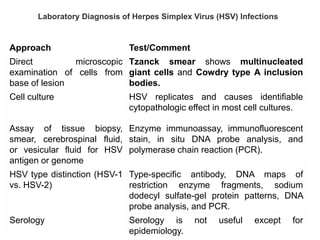
Laboratory Diagnosis ofHerpes Simplex Virus (HSV) Infections
Approach Test/Comment
Direct microscopic
examination of cells from
base of lesion
Tzanck smear shows multinucleated
giant cells and Cowdry type A inclusion
bodies.
Cell culture HSV replicates and causes identifiable
cytopathologic effect in most cell cultures.
Assay of tissue biopsy,
smear, cerebrospinal fluid,
or vesicular fluid for HSV
antigen or genome
Enzyme immunoassay, immunofluorescent
stain, in situ DNA probe analysis, and
polymerase chain reaction (PCR).
HSV type distinction (HSV-1
vs. HSV-2)
Type-specific antibody, DNA maps of
restriction enzyme fragments, sodium
dodecyl sulfate-gel protein patterns, DNA
probe analysis, and PCR.
Serology Serology is not useful except for
epidemiology.
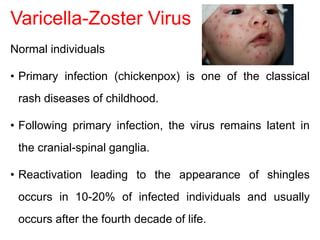
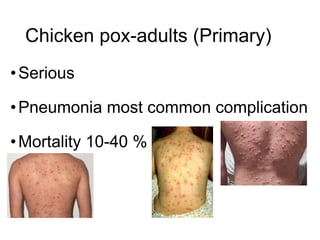
Varicella-Zoster Virus
Normal individuals
•Primary infection (chickenpox) is one of the classical
rash diseases of childhood.
• Following primary infection, the virus remains latent in
the cranial-spinal ganglia.
• Reactivation leading to the appearance of shingles
occurs in 10-20% of infected individuals and usually
occurs after the fourth decade of life.
61.
Immunocompromised individuals
Primary infection
•Severe in children -anti malignancy drugs- leukemia and
lymphoma.
• Life-threatening complications such as disseminated varicella,
pneumonia, and encephalitis are much more likely to be seen.
Reactivation
• Immunocompromised : herpes zoster, appear at an earlier
age and more than one episode may occur.
• Severe, disseminated disease may occur but fatality is rare.
62.
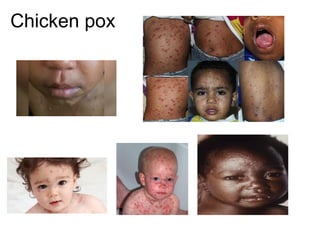
Varicella or Chickenpox
• Always acute disease
• IP 7-23 d-infectious 2 d before rash
• Rash-face, neck trunk, axillae, limbs, shoulder
blades
• Duration of disease-7 and 10 days, up to 2-4 wks
• Complications rare
• Mortality very low
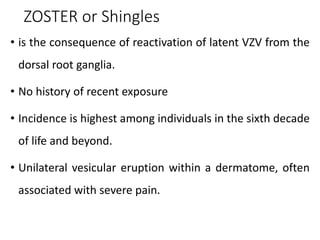
ZOSTER or Shingles
•is the consequence of reactivation of latent VZV from the
dorsal root ganglia.
• No history of recent exposure
• Incidence is highest among individuals in the sixth decade
of life and beyond.
• Unilateral vesicular eruption within a dermatome, often
associated with severe pain.
Treatment and Prevention
•Acyclovir -severe varicella or zoster infections.
• A live attenuated vaccine controversial in
Immunocompromised individuals
• VZIG can be used to prevent primary infection in
susceptible individuals.
70.
Cytomegalovirus
• The largestof the Herpes viruses, genome ~240kbp
• CMV infection is common more than 50 %
population experienced infection by the age of 40
• Most infections are asymptomatic occurs in people
except with immune defects (T-cell defects)
/pregnancy / newborns (congenital)
71.
Cytomegalovirus(CMV)
• Betaherpesvirnae: lymphotropic
•Primary target cell: monocyte, lymphocte,
epitelial cell
• Site of latency: monocyte, lymphocyte and?
• Means of spread: close contact, transfusions,
tissue transplant and congenital
72.
Sources of infection
•Neonate:transplacental transmission,
intrauterine infection, cervical secretion
•Baby or child: body secretions, breast milk,
saliva, tears, urine
•Adult: sexual transmission(semen), blood
transfusion, organ graft
73.
1. CMV: Normalindividuals
• Primary infection is usually asymptomatic
• occasionally an infectious mononucleosis-like
illness may be seen.
• Reactivations or re-infections are common
throughout life and are usually asymptomatic.
74.
2. CMV: Immunocompromisedindividuals
• Primary CMV infection is usually more severe than
recurrent infection
• with the exception of bone marrow transplant
recipients, where primary and recurrent infections
are just as severe.
75.
Immunocompromised individuals ClinicalManifestations
• Fever, Pneumonitis , Hepatitis
• Gastrointestinal manifestations e.g. colitis
• Encephalopathy
• Retinitis
• Pneumonitis is the most severe manifestation, and
carries a mortality rate of 85% in the absence of
treatment.
76.
3. CMV: AIDSPatients
• CMV disease is present in 7.4% to 30% of all AIDS
patient.
• Sight-threatening retinitis, colitis, and
encephalopathy are the most common
manifestations of CMV disease in AIDS patients.
• Pneumonitis is extremely rare.
77.
4. Congenital infection
•An important cause of congenital disease
• Maternal infection usually asymptomatic
• Serious birth defects is high if primary infection occurs
during pregnancy
• Microcephaly, intracerebral-calcification, hepato-
splenomegaly
• Rash (cytomegalic inclusion disease)
• Unilateral or bilateral hearing loss, mental retardation
Treatment (CMV)
• Ganciclovir- is the drug of choice. However, it is
associated with neutropenia and thrombocytopenia.
• Forscarnet - can be used as the 2nd line drug.
Again it is very toxic and is associated with renal
toxicity.
• Cifofovir - approved for the treatment of CMV
retinitis. It is also associated with renal toxicity.
• Fomivirsen - approved for the treatment of CMV
retinitis.
Epstein-Barr Virus-clinical……
• Primaryinfection-infected saliva
• Incubation period30-50 days
• Initiate infection in oropharynx
• Replication B cells or epithelial cells
• Most asymptomatic/ subclinical in child
83.
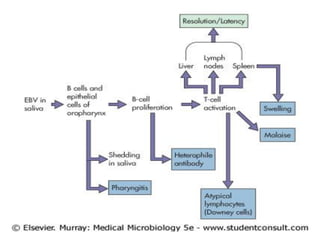
Disease Mechanisms ofEpstein-Barr Virus
•Virus in saliva initiates infection of oral epithelia
and spreads to B cells in lymphatic tissue.
•There is productive infection of epithelial and B
cells.
•Virus promotes growth of B cells (immortalizes).
•T cells kill and limit B-cell outgrowth.
•T cells are required for controlling infection.
Antibody role is limited.
84.
Disease Mechanisms ofEpstein-Barr Virus
•EBV establishes latency in memory B cells and is
reactivated when the B cell is activated.
•T-cell response (lymphocytosis) contributes to
symptoms of infectious mononucleosis.
•There is causative association with lymphoma in
immunosuppressed people and African children living
in malarial regions (African Burkitt's lymphoma) and
with nasopharyngeal carcinoma in China.
85.
Epstein-Barr Virus
• Ubiquitous
•Acute infectious mononucleosis / nasopharyngeal
carcinoma
• Burkitt’s Lymphoma and other lymphoproliferative
disorders
• Dual cell tropism for human B-lymphocytes
(generally non-productive infection) and epithelial
cells (productive infection
86.
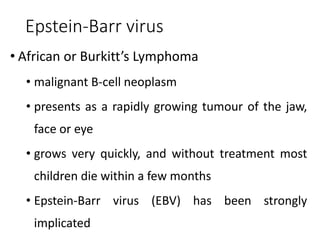
Epstein-Barr virus
• Africanor Burkitt’s Lymphoma
• malignant B-cell neoplasm
• presents as a rapidly growing tumour of the jaw,
face or eye
• grows very quickly, and without treatment most
children die within a few months
• Epstein-Barr virus (EBV) has been strongly
implicated
87.
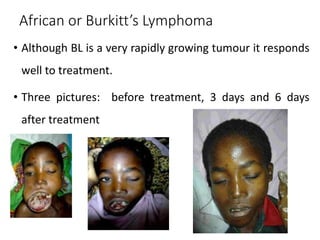
African or Burkitt’sLymphoma
• Although BL is a very rapidly growing tumour it responds
well to treatment.
• Three pictures: before treatment, 3 days and 6 days
after treatment
88.
Nasopharyngeal Carcinoma
• Endemicin South China, Africa, Arctic Eskimos
• This is a malignant tumour of the squamous epithelium of
the nasopharynx.
• Nasopharyngeal carcinomas are found in association with
reactivation of latent Epstein-Barr Virus.
• The exact mechanisms of association are unknown
89.
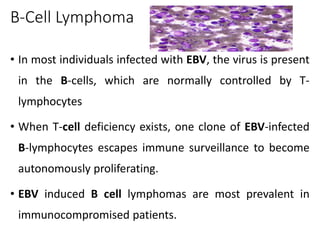
B-Cell Lymphoma
• Inmost individuals infected with EBV, the virus is present
in the B-cells, which are normally controlled by T-
lymphocytes
• When T-cell deficiency exists, one clone of EBV-infected
B-lymphocytes escapes immune surveillance to become
autonomously proliferating.
• EBV induced B cell lymphomas are most prevalent in
immunocompromised patients.
90.
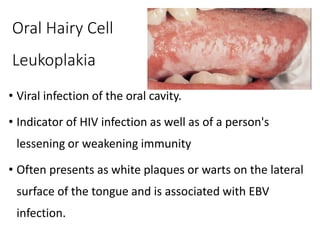
Oral Hairy Cell
Leukoplakia
•Viral infection of the oral cavity.
• Indicator of HIV infection as well as of a person's
lessening or weakening immunity
• Often presents as white plaques or warts on the lateral
surface of the tongue and is associated with EBV
infection.
91.
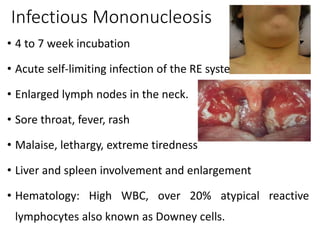
Infectious Mononucleosis
• 4to 7 week incubation
• Acute self-limiting infection of the RE system
• Enlarged lymph nodes in the neck.
• Sore throat, fever, rash
• Malaise, lethargy, extreme tiredness
• Liver and spleen involvement and enlargement
• Hematology: High WBC, over 20% atypical reactive
lymphocytes also known as Downey cells.
92.
Diagnosis
• Acute EBVinfection is usually made by the heterophil
antibody test and/or detection of anti-EBV IgM.
• Cases of NPC should be diagnosed by histology.
• The determination of the titre of anti-EBV IgA in
screening for early lesions of NPC and also for monitoring
treatment.
• PCR
93.
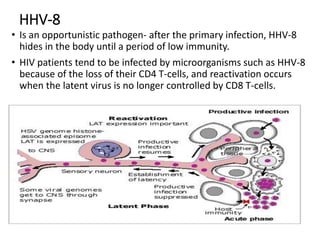
HHV-8
• Is anopportunistic pathogen- after the primary infection, HHV-8
hides in the body until a period of low immunity.
• HIV patients tend to be infected by microorganisms such as HHV-8
because of the loss of their CD4 T-cells, and reactivation occurs
when the latent virus is no longer controlled by CD8 T-cells.
94.
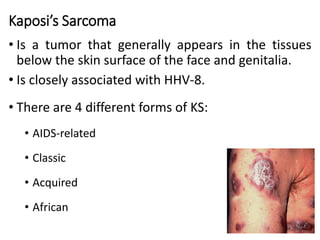
Kaposi’s Sarcoma
• Isa tumor that generally appears in the tissues
below the skin surface of the face and genitalia.
• Is closely associated with HHV-8.
• There are 4 different forms of KS:
• AIDS-related
• Classic
• Acquired
• African
95.
95
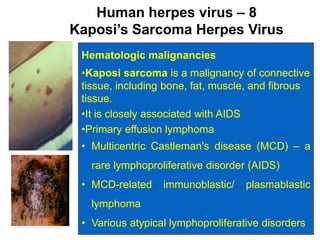
Human herpes virus– 8
Kaposi’s Sarcoma Herpes Virus
Hematologic malignancies
•Kaposi sarcoma is a malignancy of connective
tissue, including bone, fat, muscle, and fibrous
tissue.
•It is closely associated with AIDS
•Primary effusion lymphoma
• Multicentric Castleman's disease (MCD) – a
rare lymphoproliferative disorder (AIDS)
• MCD-related immunoblastic/ plasmablastic
lymphoma
• Various atypical lymphoproliferative disorders
96.
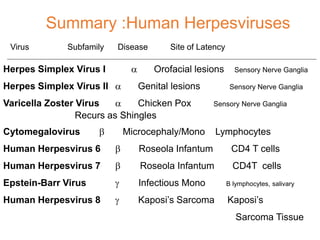
Virus Subfamily DiseaseSite of Latency
Herpes Simplex Virus I a Orofacial lesions Sensory Nerve Ganglia
Herpes Simplex Virus II a Genital lesions Sensory Nerve Ganglia
Varicella Zoster Virus a Chicken Pox Sensory Nerve Ganglia
Recurs as Shingles
Cytomegalovirus b Microcephaly/Mono Lymphocytes
Human Herpesvirus 6 b Roseola Infantum CD4 T cells
Human Herpesvirus 7 b Roseola Infantum CD4T cells
Epstein-Barr Virus g Infectious Mono B lymphocytes, salivary
Human Herpesvirus 8 g Kaposi’s Sarcoma Kaposi’s
Sarcoma Tissue
Summary :Human Herpesviruses
HPV…
Properties
• Genome iscircular ds DNA
• More than 80 types of HPV
• Non-enveloped with icosahedral symmetry
• Possess capsomeres surround the genome
98
99.
• Three majorregions comprise the HPV genome :
Early region (E1-8) consists of genes responsible for
transcription & transformation
The late region codes for the major (L1) and minor
(L2) capsid proteins &
Control region contain the regulatory elements for
transcription and replication
• Replication is in host cell nucleus
• Undergo cell transformation
99
Epidemiology ; HPVprevalence
• There is regional & ethnic variation in HPV types
• HPV 16,18,33 and 45 are mostly found in cervical cancers
worldwide
• HPV 16 & 18
• present in 50% & 20% of all cases respectively
• are predominant types in newborns
• Types 6 and 11 are commonly associate with genital warts
(Condyloma acuminatum)
• Types 2,4,29 & 57 occur in common skin warts
• No complete data on HPV prevalence in developing countries
102
Transmission
1. Sexual contact
•Grater than 95% of infection
• In children associated with sexual abuse
2.Vertical transmission
Less frequent mode of transmission
Difficult to detect due to the latency period
3. Other pathways
• e.g. contact with infected urogenital secretions or bathing
together
104
105.
Risk factors forHPV
1. Sexual behavior
• Is a primary risk factor for infection
• Women with multiple sex partners have a higher risk than
monogamous women
2. Immune suppression
• A person with a pre-existing immuno-compromised state
and/or concurrent genital infection has a 17-fold increased
risk of developing the diseases
105
106.
• A strongassociation of E6 and/or E7 with cervical
carcinoma was observed among Ethiopian cervical cancer
patients as well, with 72.7% positives
• Increased risk of HPV in people with HIV infection
• The HIV+ women also had higher rates of oncogenic HPV types,
which progressed to cancer
106
107.
3. Age
• Youngwomen, between the ages of 15 and 25 have a two
fold higher risk of developing an HPV infection than women
over 35
4. Other possible risk factors
• Pregnancy, smoking , concurrent herpes infections , others
5. Socioeconomic variables
• Poverty, domestic violence, sexual abuse, inadequate
health Care & lack of information
►Can facilitate disease transmission , prevent early detection &
treatment
107
Human Parvoviruses
•Parvoviruses arethe smallest viruses
►In Latin, parvum meaning small
• Posses ssDNA genome
• One known human pathogen (parvovirus
B19)
111.
Human parvovirus B19(B19V)
Structure
Non-enveloped and Icoashedral
As with all parvovirus particles, B19V:
Stable over a wide range of pH
Resistant to lipid solvents
Not quite resistant to heat as other parvoviruses
Inactivated by formalin, oxidizing agents & γ-
irradiation
B19V Infection inPregnancy
• Maternal B19 infections usually do not adversely
affect the fetus
• It is estimated that fewer than 10% of maternal B19
infections in the first 20 weeks of pregnancy lead to
fetal death
115.
Laboratory diagnosis
Specimens:
Serum(principal specimen) , Tissue biopsy
A. Virus Detection :Culture
B. Serologic tests
• ELISA (detection of B19-specific IgM & IgG antibodies)
• Haemagglutination-based assays
C. Molecular technique
• Detection of viral DNA by quantitative PCR is the mainstay of
detection of B19
116.
Treatment
No specific treatmentfor B19V infection
• Except intravenous administration of human Ig in cases of
persistent infection in immuno-compromised patient
• No vaccine for B19 is currently available
Prevention and control
• Isolating of susceptible individuals …. If possible
• Vaccination of animals to prevent animal B19V































![GROUP_PRESENTATIONS poxiviridea virus1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/grouppresentations1-241003104337-bfd18a48-thumbnail.jpg?width=640&height=640&fit=bounds)




































