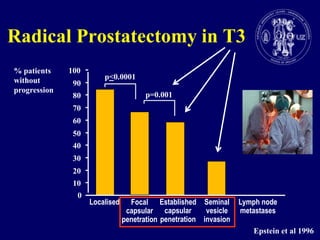
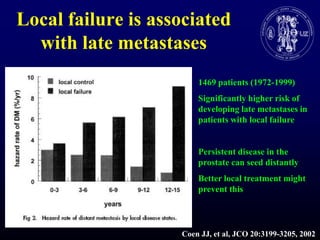
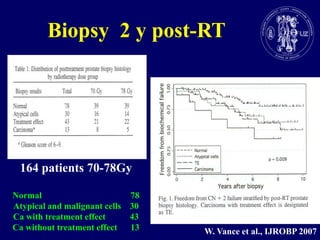
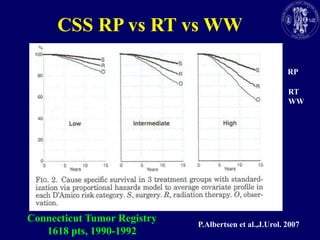
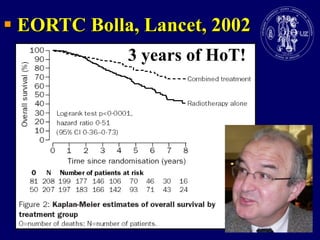
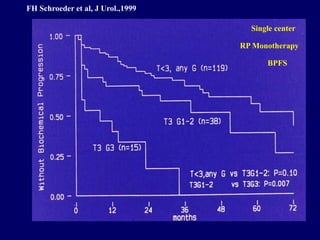
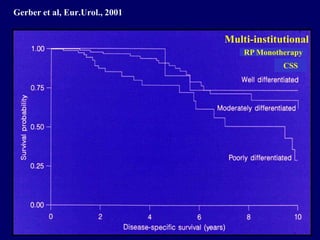
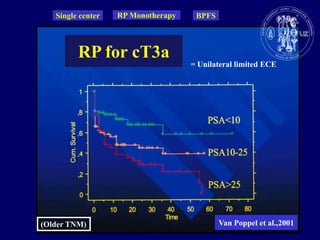
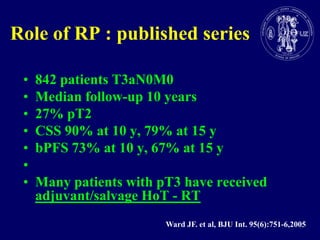
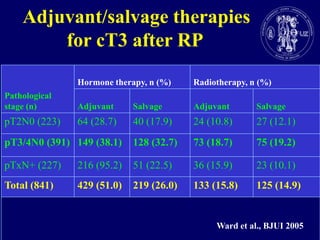
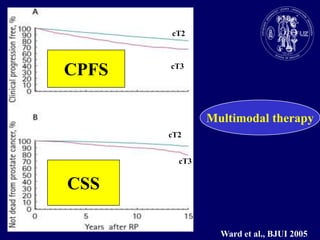
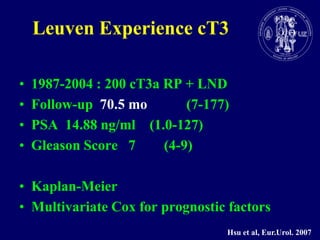
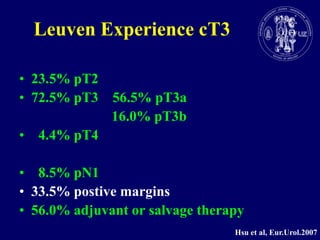
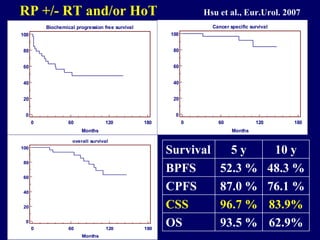
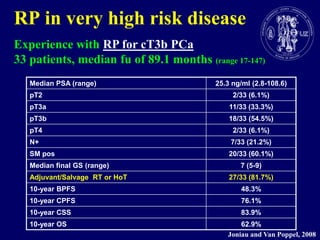
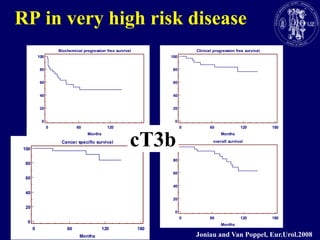
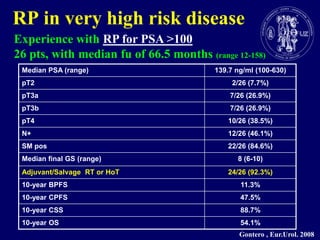
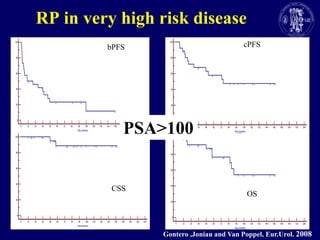
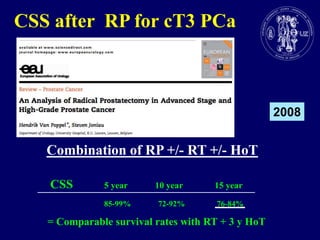
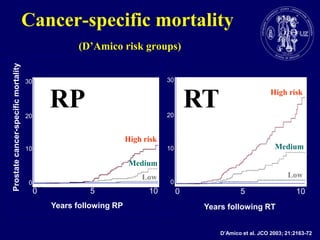
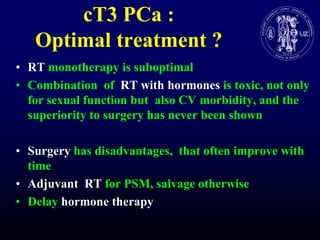

This document discusses treatment options for locally advanced prostate cancer (cT3). It finds that radical prostatectomy (RP) yields the best local control and may prevent late metastases by destroying all cancer cells. While RP alone can cure overstaged (pT2) cancers and some with extracapsular extension, many cT3 patients require adjuvant or salvage radiation therapy (RT) or hormone therapy (HoT). Studies show RP with adjuvant/salvage RT and/or HoT can achieve comparable cancer-specific survival to RT plus long-term HoT, even for high-risk cT3 cancers. Therefore, the document concludes surgery has a role, even in high-risk cT3 prostate cancer, with other