วัณโรคปอด
21
บทที่
2
เอกสารอ้างอิง
1. American ThoracicSociety/Centers for Disease Control and Prevention/
Infectious Diseases Society of America: Treatment of Tuberculosis Am J Respir Crit Care
Med 2003;67:603 - 62.
2. World Health Organization. Treatment of tuberculosis: Guidelines for national
programmes 3rd
edition 2003. (WHO/CDS/TB/2003.313) Geneva: WHO;2003.
3. WorldHealthOrganization.Treatmentoftuberculosis:Guidelines4th
edition2009.
(WHO/HTM/TB/2009.420) Geneva: WHO;2009.
วัณโรคนอกปอด
25
บทที่
3
ตารางที่ 7 ลักษณะจำ�เพาะของนํ้าจากอวัยวะที่สงสัยวัณโรค
Appearance
pH
Cellcount
Cell
differential
Protein
Glucose
Cytology
Pleural effusion
usually straw
colored
rarely < 7.3,
never > 7.4
1,000 – 5,000
lymphocytes
50–90%,
eosinophils < 5%,
few mesothelial
cells
usually > 2.5 g/dL
usually < serum
conc.
no malignant cell
Pericardial effusion
straw colored or
serosanguinous
not well described
not well described
increased lymphocytes,
PMN predominate early,
latermononuclear
cells predominate
usually high
low
no malignant cell
CSF
clear early, turbid
with chronicity
not well described
100 – 500
PMN predominate
early, later
mononuclear cells
predominate
usually high
(100-500 mg/dL)
usually less than
40-50 mg/dL
(50% of blood glucose)
no malignant cell
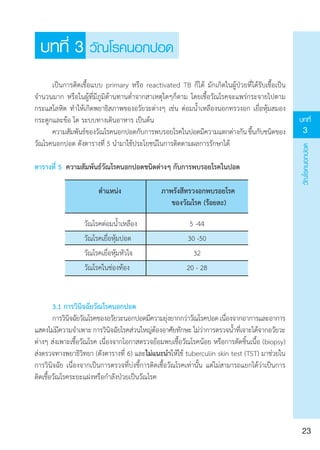
• ควรตัดชิ้นเนื้อส่งตรวจทางพยาธิวิทยา ในกรณีดังต่อไปนี้ (เว้นแต่มีหนอง ให้ใช้เข็มเจาะ
ดูดหนองส่งตรวจย้อม โดยไม่ต้องตัดชิ้นเนื้อส่งตรวจ)
o ต่อมนํ้าเหลือง
o ผิวหนัง
o กระดูกและข้อ
o อวัยวะในช่องท้อง เช่น เยื่อบุช่องท้อง
• นำ�สิ่งส่งตรวจจากอวัยวะที่สงสัยวัณโรคเพาะเชื้อวัณโรคและทดสอบความไวของเชื้อ
วัณโรคต่อยา เพื่อยืนยันการวินิจฉัยทุกราย
• การตรวจทางอณูชีววิทยา(nucleicacidamplificationtest;NAAT)เช่นPCR,real-time
PCR เป็นต้น อาจนำ�มาช่วยในการวินิจฉัยวัณโรคได้ในกรณีที่ไม่สามารถให้การวินิจฉัยด้วยแนวทาง
ตามมาตรฐาน
ยารักษาวัณโรคแนวที่หนึ่ง
36
บทที่
4
เอกสารอ้างอิง
1. American ThoracicSociety, Centers of Disease Control and Prevention, and
Infectious Diseases Society of America (2003) Treatment of tuberculosis. MMWR 52.
2. An official ATS statement: Hepatotoxicity of antituberculosis therapy.
Am J Respir Crit Care Med 2006;174:935-52.
3. Ethambutol efficacy and toxicity; literature review and recommendations for
daily and intermittent dosage in children. WHO/HTM/TB/2006.365.
4. Lode H, Rebhan K, Schaberg T. Risk for side-effects of isoniazid, rifampin and
pyrazinamide in patient hospitalized for pulmonary tuberculosis. Eur Respir J
1996;9:2026-30.
5. Luna JAC. A tuberculosis guide for specialist physicians 2004. International
Union Against Tuberculosis and Lung Disease (IUATLD).
6. Sharma SK, Singla R, Sarda P, et al. Safety of 3 different reintroduction regimens
of antituberculosis drugs after development of antituberculosis treatment-induced
hepatotoxicity. Clin Infect Dis 2010;50:833-9.
7. Talbert Estlin KA, Sadun AA. Risk factors for ethambutol optic toxicity.
Int Ophthalmol 2010;30:63-72.
8. Yee D, Valiquette C, Pelletier M, et al. Incidence of serious side effects from
first-line antituberculosis drugs among patients treated for active tuberculosis.
Am J Respir Crit Care Med 2003;167:1472-7.
การรักษาผู้ป่วยวัณโรคในกรณีพิเศษต่างๆ
42
บทที่
5
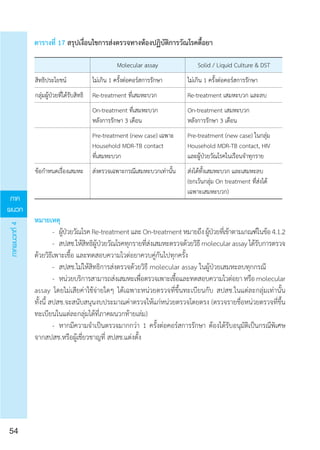
• หลีกเลี่ยงการให้ยาaminoglycosides ในหญิงตั้งครรภ์ และให้นมบุตรด้วย เนื่องจากเกิด
พิษต่อหู (ototoxic) ของทารกในครรภ์ (++, III)
• หลีกเลี่ยงยากลุ่ม fluoroquinolone ในหญิงตั้งครรภ์ และให้นมบุตร ถ้ามีความจำ�เป็นต้อง
ใช้ ควรปรึกษาแพทย์ผู้เชี่ยวชาญ เพื่อพิจารณาร่วมกับผู้ป่วยและญาติเป็นรายๆไป (++, III)
เอกสารอ้างอิง
1. Abouya L, Coulibaly IM, Coulibaly D, Kassim S, Ackah A, Greenberg AE, et al.
Radiologic manifestations ofpulmonary tuberculosis inHIV-1 andHIV-2-infected patients
in Abidjan, Cote d'Ivoire. Tuber Lung Dis 1995;76:436-40.
2. American Thoracic Society/Centers for Disease Control and Prevention/
Infectious Diseases Society of America. Treatment of tuberculosis. Am J Respir Crit Care
Med 2003;167:602-62.
3. Barnes PF, Lakey DL, Burman WJ. Tuberculosis in patients with HIV infection.
Infect Dis Clin North Am 2002;16:107-26.
4. Havlir DV, Barnes PF. Tuberculosis in patients with human immunodeficiency
virus infection. N Engl J Med 1999;340:367-73.
5. Jones BE, Young SM, Antoniskis D. Relationship of the manifestations
of tuberculosis to CD4 cell counts in patients with human immunodeficiency virus
infection. Am Rev Respir Dis 1993;148:1292-7.
6. Marries A, Maher D, Graham S, editors. TB/HIV a clinical manual, 2nd
ed., WHO 2004.
7. World Health Organization. Treatment of tuberculosis guidelines. 4th
ed.,
2010.3. An Official ATS Statement: Hepatotoxicity of Antituberculosis Therapy. Am J
Respir Crit Care Med 2006;174:935-52.
8. วินัย รัตนสุวรรณ โรคติดเชื้อ Mycobacteria ในผู้ป่วยเอชไอวีและเอดส์ ใน: พรรณทิพย์
ฉายากุล, ชิษณุ พันธุ์เจริญ, ชุษณา สวนกระต่าย, สุรภี เทียนกริม, ยุพิน ศุพุทธมงคล, ศศิธร ลิขิตนุกูล,
บรรณาธิการ. ตำ�ราโรคติดเชื้อ, พิมพ์ครั้งที่ 1 กรุงเทพฯ: โฮลิสติก พับลิชชิ่ง, 2548, 1177-91.